Madhulika Bhatia* | Amrinder Kaur | Shaveta Bhatia | Mridula | Pallavi Dwivedi
© 2022 IIETA. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Patients with Alzheimer's infection (AD) and Parkinson's sickness (PD) regularly have cover in clinical show and cognitive neuropathology proposing that these two illnesses share basic fundamental instruments. Parkinson sickness emerges from diminished dopamine creation in the mind. Patients with these two illnesses often cover in clinical introduction and cerebrum neuropathology proposing that they share basic common fundamental systems. Therefore, it become important two find the presence of common affected brain region of interest. The paper proposes the technique to find out the relation between the common affected brain areas. The work with in carried in-depth analysis of brain functional MRI scans using statistical parametric mapping on both AD, PD patients (n=35), which comprises of 5 healthy participants with average age 83, 5 AD participants with average age 75, Early mild cognitive impairment (EMCI) participants whose average age is 65, Late mild cognitive impairment (EMCI) participants whose average age is 75 and PD participants with average age of 64. Using a two sample t-test the ROI (region of interest) was noted using MarsBar plugin of SPM tool.
Parkinson's disease, MRI, SPM, MarsBar
Alzheimer’s illness (AD), Parkinson’s illness (PD) are most basic neurological issues which are portrayed by the disturbance of standard activities of mind capacities. A patient with both of these NLD puts a weighty weight on the family, therefore it is important to identify these issues at the soonest stage with the goal that their movement can be eased back down, if not completely halted. The shortfall of dopamine makes it difficult for the mind to arrange muscle developments. Low dopamine additionally adds to disposition and intellectual issues later throughout the illness. Specialists don’t have a clue what triggers the improvement of Parkinson sickness more often than not. Almost 60-80% of dementia cases rep resent Alzheimer’s infection. It deteriorates after some time. Alzheimer’s has no 100% cure, yet medicines for manifestations are accessible and research proceeds. The current Alzheimer’s medicines can’t prevent it from advancing, they can briefly lethargic the deteriorating of dementia manifestations and improve personal satisfaction for those with Alzheimer’s and their guardians. Neurodegenerative issues influence around one billion individuals around the world. They can emerge from a blend of genomic, epigenomic, metabolic, and ecological variables. Maturing is the main danger factor for most constant sick- nesses of mature age, including Parkinson’s and Alzheimer’s illnesses [1].
Other conceivable perception difficulties can incorporate depression. While not generally a crisis, misery can likewise cause a to some degree unexpected change in individuals’ psychological capacity. Dementia is the first stage of AD. Hereditary and natural variables including diet, action, smoking, awful cerebrum injury, diabetes, and other clinical illnesses add to the danger of fostering this type of the sickness. The indication of dementia can incorporate at least one from a rundown that incorporates memory disappointment, decreased capacity to remember numerous assignments at the same time and split consideration between them, issues with language appreciation or articulation, inconvenience understanding spatial direction, debilitated chief capacity, and off base deciphering of others’ nonverbal signs. Most of individuals with AD have the late-beginning sort-where manifestations initially show up after the mid-60s. PD starts sooner than AD, normally between ages 50 and 65, with a normal time of beginning of around 62 years, and a couple of cases start before age 40. With a predominance of around 3 cases for each 1,000 individuals, PD is more uncommon than AD yet a significant reason for neurological disease among more established grown-ups. Like the indications of AD, those of PD are brought about by obliteration of synapses. In contrast to AD, in which plaques and tangles are tracked down, the infinitesimal finding in PD minds is loss of cells that produce dopamine, a significant cerebrum synthetic engaged with nerve cell correspondence, in a development related piece of the cerebrum called the substantia nigra [2]. The middle cross section of fMRI is shown in Figure 1. The phones in the substantia nigra can be believed to incorporate unusual assortments of a protein, called” Lewy bodies.” There are three cardinal cycles of atomic pathogenesis like proteinopathy, mitochondrial dysfunction and oxidative pressure role in PD and AD. These three harm components work in show, supporting each other to drive the pathology in the maturing mind for both the infections; curiously, the idea of associations among these three harm systems is basically the same in both the sicknesses, and this survey endeavors to feature these perspectives [3].
Figure 1. A middle cross-section of fMRI data a Parkinson’s brain (left), and an Alzheimer’s brain is shown (right)
The symptoms generally start continuously and deteriorate after some time. As the disease progresses, individuals may experience issues strolling and talking. Parkin- son’s influences synapses that produce dopamine, a significant mind synthetic including nerve cell correspondence. Dopamine lives in a piece of the mind called the substantia nigra, a design in the cerebrum that assumes a part in remuneration in development. As the illness advances, individuals may experience issues strolling and talking. The most well-known introductory treatment for patients is Levodopa, a prodrug to dopamine [4]. Parkinson’s is something beyond a development issue, and the non-engine indications can frequently be more weakening than the quakes or dyskinesia. It has distinguished neuropathological cerebrum changes. There is the development of strange proteinaceous round bodies called Lewy bodies, and a spindle string-like and, to a limited extent, spreading Lewy neurites in the somata of the elaborate nerve cells, starting at characterized acceptance locales and progressing in a geologically unsurprising grouping inside the sensory system. The beginning of the infection is ordinarily at an age of 65 to 70 years. Beginning before the age of 40 is seen in under 5% of the cases in populace- based accomplices. Parkinson’s infection (PD) is portrayed by its primary motor side effects bradykinesia, inflexibility, and tremor, yet in addition, has extra motor and non-motor attributes [5].
2.1 (fMRI) images
The “functional Magnetic Resonance Imaging” (fMRI) is a particular kind of attractive reverberation imaging that exclusively centers around the little metabolic changes that occur while utilizing a particular locale of the brain. It is to identify restricted changes in blood stream and blood oxygenation in the mind that happen in reaction to neural movement. Studies have utilized resting-state useful attractive reverberation imaging (rs-fMRI) to look at relationship among psychopathy and mind availability in chose districts of interest just as organizations covering the entire cerebrum [6].
2.2 Alzheimer's disease
Alzheimer’s infection begins in the hippocampus, profound inside and part of the worldly projection of the cerebrum. It unmistakably exhibits a tangled condition with an assortment of atomic variations from the norm, prompting the possible introduction of the illness. The hippocampus is the structure liable for making new recollections from our encounters. Plaques structure when protein pieces called beta- cluster together. Beta-amyloid comes from a bigger protein found in the greasy layer encompassing nerve cells. The most prominent early detection of disease even without showing symptoms is get test with plaques, tangles formed in brain region. Alzheimer’s upsets measure imperative to neurons and their organizations [6], in-clouding correspondence, digestion, and fix. The disease moves from hippocampus to cerebral cortex reaching the temporal lobes, which play a crucial role in transforming language and sounds. In later stages of disease cortex gets destroyed completely and a person lose their ability of recognition, commination taking care of themselves.
The three stages of Alzheimer’s Disease:
Also, Alzheimer’s is a progressive disease and in the later stages of the it is difficult to treat. The way to present for finding relationship between AD and PD using fMRI scans and the brain region of the patients suffering from Alzheimer’s having PD is highlighted. In progression from mild to direct stages, mind locales significant in memory and thinking and arranging foster a greater number of plaques and tangles than were available in beginning phases. Accordingly, people foster issues with memory or thinking adequately genuine to meddle with work or public activity. They may likewise get befuddled and experience difficulty taking care of cash, putting themselves out there and coordinating their musings. Numerous individuals with Alzheimer’s are first analyzed in quite a while. In late stages or severe AD most of the cortex is destroyed, the brain gets shrink due to major cell death and patients lose their thinking ability, communication ability, recognition rate is also decreased.
Lin et al. [8] reviewed the most mainstream DL strategies have been investigated in distinguishing those three driving neurological issues Alzheimer’s disease, Parkinson’s disease and schizophrenia from the MRI scans. DL techniques for the characterization of neurological have been discussed and the pros, cons, and execution of these DL methods for the neuroimaging information have been summed up. Also, the open difficulties and future patterns have been examined. The Prime perception of this investigation incorporated the most extreme utilization of CNN in the discovery of Alzheimer’s sickness and Parkinson’s illness.
Singleton and Hardy [9] objective was to study subjective cognitive decline (SCD) on a local area based along with clinical 2978 samples suffering with SCD and 1391 healthy controls so that to find the occurrence of AD infection, non-AD dementia and to determine the reason for progression of dementia.
Ball et al. [10] designed a framework applying deep convolutional neural network (DCNN), to estimate MCI-to- AD transformation using magnetic resonance imaging (MRI). The methodology involves firstly MRI pictures were set up according to age. Second, nearby fixes, which are collected into 2.5 measurements, are extricated from these pictures. At that point, the patches from AD and typical controls (NC) are utilized to prepare a CNN to recognize profound learning highlights of MCI subjects. From that point onward, underlying brain region highlights are mined with Free Surfer to help CNN. At long last, both sorts of highlights are taken care of into a limit learning machine classifier to foresee the AD change. The results show an accuracy of 79.9% in predicting features of hippocampus gyrus.
Analysing the role of genetics and its challenges in research in neurogenerative diseases. The methodology has fixated on the thought that distinguishing quality changes will at last permit us to comprehend the sub-atomic cycles that start and support the infection pathogenesis.
Hanagasi et al. [11] examined the part in which demographical/natural factors that may affect the seriousness of the Parkinson sickness. By understanding the systems in which ecological elements interface with, and influence the cerebrum we can walk toward finding the hidden causes of PD.
Raza and Anjum [12] surveyed recent trends to the current arrangement, the board techniques and the Parkinson’s illness models for translational examination. Preclinical exploration may give amazing assets to mission the expected helpful and neuroprotective mixtures for dopaminergic neurons and henceforth conceivable remedy for the Parkinson’s infection.
Fiorenzato et al. [13] studied 118 patients MRI scans (n=46 MCI, n= 52 CN, n=20 dementia) to distinguish contrasts in the unique network across Parkinson’s illness state of cognition, going from typical comprehension to dementia, with an attention on the transient properties. To study the dynamic functional connectivity a sliding window approach resting state functional MRI. The investigation demonstrates that dementia in Parkinson’s infection is de- scribed by modified worldly properties in dynamic network. It concluded show that expanded stay time in the isolated state and decreased number of changes between states are related with presence of dementia in Parkinson’s sickness.
Lott and Head [14] overviewed the latest research works, emerging technologies and predicted that neuroimaging is not very effective measure in predicting dementia in Parkinson’s illness. Moreover, the recent methods are delicate towards tissue microstructure/ biochemical changes that mirror the most punctual phases of the cognitive association which are presently turning out to be accessible. The conclusion was made that MRI approaches can evaluate attractive weakness as a substitute for tissue iron substance, and progressively amazing numerical methodologies can describe the geography of mind networks at the frameworks level for example, ligands that tie to tau and amyloid, and may include multimodal approaches. They should be explicitly tried longitudinally in huge scope investigations of patients with Parkinson’s infection to survey their job in early recognition of psychological inclusion and at last in anticipating Parkinson’s dementia.
Lanskey et al. [15] used Tandem Mass Tag isobaric naming and coordinated antecedent choice based MS3 (SPS-MS3) mass spectrometry to perform impartial quantitative investigation of human cerebrum tissues on 80 people of different groups characterized as controls, AD, PD, and co-horrible AD/PD cases across two brain districts i.e.: cerebrum and foremost cingulate gyrus. The conclusion was made that this research is good source for future researchers. However, it does not identify any particular protein and molecule combination that are common in Parkinson’s Alzheimer’s disease.
Ping et al. [16] explores the molecular link between AD, dementia, cognitive decline and Presbycusis. It is concluded that ARHL (age-related hearing loss) can be a Risk Factor for Cognitive Decline, Dementia or AD, the particular sub-atomic com- ponent connecting these ailments is at this point unclear. It is likewise still not satisfactory whether the relationship is unidirectional or bidirectional or on the off chance that they are both the clinical indications of maturing.
Shen et al. [17] investigated the enlargement or the diminished movement in default mode network action examining changes in hippocampal connectivity in early AD and offers a sign to decreased uprightness in hippocampus-related organizations in right on time AD using fMRI imaging. A total of 28 participants were taken in total where 14 were healthy controls and 14 were suffering from Alzheimer’s.
Wang et al. [18] explored the mode network of brain using fMRI scans and modification was found in the brain anterior frontal, posterior cingulate cortex and precuneus. The study was carried on 18 patients suffering with AD, 41 healthy controls 28 patients suffering from mild cognitive impairment (MCI) and inactivation was detected in default mode network of different brain areas. This research discovered that in healthy controls defusing in a typical organization including foremost frontal projection what’s more, precuneus and back cingulate cortex whereas in AD and MCI patients indicated adjustments in this default mode network which was generally articulated in the early period of deactivation.
Rombouts et al. [19] examined whether Alzheimer’s disease in late life depression is associated with lower hippocampal volume on 100 participants who went under MRI. The results confirmed that patients with late- life depression hippocampal volume is smaller in comparison with healthy comparison subjects. The main examination is that lower hippocampal volume was not because of a further extent of amyloid affidavit in the late-life melancholy gathering and it was also not discovered any relationship between hippocampal volume and amyloid accumulation in patients.
De Winter et al. [20] goal was to create and assess a classifier for separating plausible Alzheimer’s illness (AD) from Parkinson’s infection or dementia with Lewy bodies. Using the quantitative electroencephalography QEEG features the classification achieved an accuracy, sensitivity, and specificity of 100%.
Kumar et al. [21] conducted a sub proteomic examination of membrane-enriched post-mortem brain examples AD. A total of 6 samples were taken and 14 modules of corelations with brain activity were analysed. The author concluded that system based analysis of brain proteome produced network associated with brain anatomy, in future the study of this membrane may help researchers to solve complex stage Alzheimer’s.
Espinoza et al. [22] proposed approach fuses adequately one-sided neural organization usefulness and permits a dependable Alzheimer’s infection acknowledgment. In correlation with ordinary classifiers relies upon time arrangement R-fMRI results, the proposed profound learning calculation has improved fundamentally and, in the best cases, the standard deviation decreased by 45%, demonstrating the figure model is more solid and effective according to regular philosophies. The work inspects the advantages of improved profound taking in calculations from perceiving high-dimensional data in medical care and can prompt the early analysis and avoidance of Alzheimer’s infection. The procedure proposed increments analytic precision by roughly 25% contrasted and conventional methodologies, which means consolidating the cerebrum with improved profound learning is an amazing method to analyse neurological issues early. The model preparing and information grouping utilizes all FMRI pictures and messages, including age, sex and hereditary qualities. In view of the R-fMRI signal connection, practical scholarly organizations are assembled and afterward utilized for improved neural organization development as relationship coefficient data.
Johnson et al. [23] study proposes that rt fMRI neurofeedback preparing standards are plausible in patients of Cushion and in the solid older and might be utilized to balance intellectual impacts of both AD and sound maturing. The study was conducted on 19 patients: 10 patients of PD suffering with MCI 13 HCI patients. The author concluded cognitive decline is present in AD with MCI, also an activity in frontal gyrus. Sveinbjornsdottir [24] inspected the remodelling of global synchronizations of brain activities and the neural correlations of cognitive and movement function in PD patients is investigated is performed on 90 patients (30 HC, 30 PD) using fMRI scans. Degree centrality (DC) and cognitive function Frontal Assessment Battery (FAB) were measured using a PD rating scale and correlation between neurons is also identified. The inference is made that in identification of cognitive functions in PD the regions of brain connectivity are fusiform gyrus, hippocampus gyrus, cerebellum.
Tysnes and Storstein [25] studied the affected brain areas in PD patients when they face visual hallucinations at progressive disease state. A total of 9 patients were enrolled for this study plus a two- step research is performed. Firstly, a data-based analysis of patients pre hallucination fMRI data. Secondly, a post fMRI scans exploration in order to find out the brain components affected. The recommendation from this study is that visual hallucinations in PD relates to broken actuations of mental portrayals, a finding likewise viable with the way that the network between significant segments of the visual ventral stream that intervenes the change of visual sign into mental Cerebrum Imaging and Behaviour portrayals was expanded in visual hallucinations.
Dwivedi et al. [26] discussed the role of Tau protein in PD. The review stated the fact that there is no compelling treatment or medication treatment for PD and other comparable neurodegenerative illnesses, understanding the design, capacity, and system of tau and tau pathology may be useful for early conclusion and treatment of PD in the future.
Garn et al. [27] presented the first comprehensive study on the damage of connectivity in substantia nigra and axonal in early PD using positron emission tomography (PET) scans. The evaluation was performed on (n=36 idiopathic PD patients, 14 HC), also the disease severity was measured using the Unified Parkinson’s disease Rating Scale (UPDRS). Chi- squared, t-test have been used to identify demographic differences. The outcome of this study shows a remarkable axonal presynaptic degeneration in the PD patients and extreme in nigra [28].
4.1 Subjects
The investigational data was gathered from the Alzheimer’s Disease Neuroimaging Initiative (ADNI) (http://adni.loni.usc.edu/) dataset which incorporates an assortment of neuroimaging information for AD patients. The ADNI study was supported by Institutional Review Board (IRB) of each taking part site. All ADNI subjects along with their lawful agents ought to have composed educated assent prior to gathering clinical, hereditary and imaging information [29, 30]. The PD patient’s data was collected from Parkinson’s progression markers initiative (PPMI) (http://www.ppmi- info.org/). PPMI is a milestone observational examination to all the more likely characterize and measure Parkinson’s sickness to speed remedial turn of events. PPMI makes its informational collection and biorepository-the most vigorous in Parkinson’s to date-accessible to the scholarly world and industry to speed up forward leaps. The criteria for data collection were to select subjects whose scans must be in resting state fMRI state for both the categories. At last, 35 subjects were selected, comprising of 14 AD, 16 PD, 5 HC (Healthy Controls) [31, 32].
A. Data collection and preprocessing
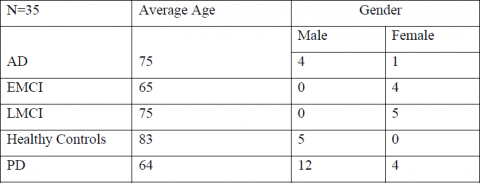
The fMRI images need to be pre-processed to decrease the effect of signal to noise ratio. Therefore, the images were re- aligned registered, normalized and smoothening was done to accomplish uniform resolution. These fMRI images were pre- processed using Statistical Parametric Mapping 12(SPM12) tool by MATLAB 2019b on windows operating system. 35 participants were included in this study, comprising of 5 healthy patients [33], 4 Early mild cognitive impairment (EMCI), 5 Late mild cognitive impairment (LMCI), 5 Alzheimer’s and 16) Parkinson’s patients. On all the participants, six parameter transformation of images is done using realignment, voxel-to- voxel relative change network is shown using Coregistration, then images were normalized, matching scans to a template across subjects is done using Normalization and to adjust the residual differences and alignment errors Smoothing was performed. Demographics are shown in Figure 2.
Figure 2. Demographics of AD, AD-EMCI, AD-LMCI, PD, HC groups
B. Proposed work
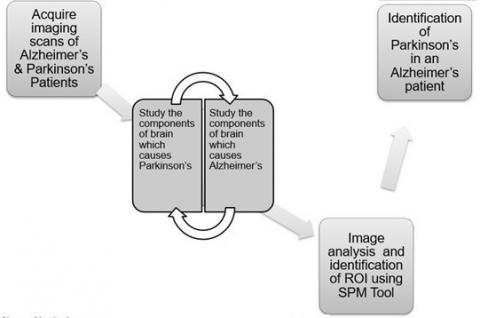
In this work, we performed a semantic analysis of fMRI scans of patients who are in different stages AD disease and simultaneously for PD disease in order to refine the knowledge of disease in respective of AD and vice-versa. After acquiring information from ADNI data set, we performed picture preparing, we removed volume, surface also, voxel highlights across various mind territories divided [34, 35]. Similarly, after collection data from PPMI dataset, we performed all the pre-processing steps on the scans of PD affected people. We then studied and analysed the components of brain which causes PD along with the components which causes Alzheimer’s and examined the relationship between both the maladies. After that, we investigated the region of interest in the fMRI scans as well as found the common brain regions affected by both the diseases [36, 37]. The proposed word is shown in Figure 3.
Figure 3. An overview of the proposed work
Figure 4. Methodology flowchart
In our work, fMRI images were acquired from ADNI PPMI dataset. We took datasets of PD, LMCI, AD, EMCI and Healthy controls patients. All the images of patients were then pre-processed using SPM tool [38] in order to get that same orientation of brain in all images. The fMRI images were re- aligned coregistered, normalised and smoothening was done to accomplish uniform resolution [39]. These fMRI images were pre- processed using Statistical Parametric Mapping 12(SPM12) tool by MATLAB 2019b on windows operating system. The detailed representation in the flow chart for the proposed method is shown in Figure 4.
The demographic details of all the 35 participants are shared in Table 1 (see Appendix). There was no significant difference among the three groups in gender, age of subjects. A two-sample t-test with p-value of 0.05 was conducted and then all EMCI, LMCI, AD, PD patients’ images were compared with Healthy control patients [40, 41] and affected regions the functional connectivity of brain is then explored. The goal is to study relation between Alzheimer’s Parkinson’s and to identify the common brain regions. The statistical analysis was done using statistical para- metric modelling and a single session was run on five patients, the parameters taken are age, and a constant threshold of p ¡ 0.05 and a design is being prepared and shown in Figure 5. The functional connectivity is shown in Figure 6.
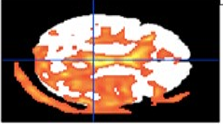
The lower performance was seen in PD patients in comparison with controls. No critical contrasts were noted at right foremost cingulate cortex, inferring unblemished capacities in AD patients [42, 43]. The patients suffering with PD and severe AD were having less brain activity in cingulate cortex amygdala and hippocampus were coloured red as shown in Figure 7.
Figure 5. The functional connectivity of brain regions
Figure 6. (a) SPM results
Height Threshold T=156.279 p<0.05
Figure 7. EMCI patients
Figure 8. (a) Height Threshold T=6.75 p<0.05
Figure 8. (b) Design matrix
Figure 9. Brain model
Two sets of tests were conducted one was of AD patients and healthy patients. In addition to this AD tests were divided into the sets of EMCI, LMCI diseased patients against healthy controls. Second was conducted with Parkinson’s sick person with HC. To identify the Region of interest (ROI) a plugin called MarsBar used with SPM toolbox.
The performed test with EMCI patients against same healthy controls under same p-value (p =0.05) the observation was made that the area which were affected were entorhinal cortex and hippocampus and most of the regions were highlighted with yellow colour in Figure 8. EMCI patients against same healthy controls under same p-value is shown in Figure 9.
Prefrontal cerebrum hindrance is extraordinary compared to other imitated hazard factors for forceful conduct. In last decades there has been a quick expansion in fMRI concentrates in psychopathy, and meta-logical discoveries has featured decreases in the privilege orbitofrontal cortex, right foremost cingulate cortex, and left dorsolateral prefrontal cortex [44]. Depression is considered as first stage of Alzheimer’s whereas in Parkinson’s there is no first stage, the disease progress at exponentially rate and it can be diagnosed only when severe symptoms are present in patient. In gentle to direct stages, cerebrum locales significant in memory and thinking and arranging grow a greater number of plaques and tangles than were available in beginning phases. Therefore, people create issues with memory or thinking sufficiently genuine to meddle with work or public activity. We analyzed individual resting-state practical connections to a gathering normal over the whole cortex from previous work and found that changes were present in both front and back cingulate cortex (ACC) [45]. The decline of cognition state is basic in both AD and PD, however essentially more uncommon in PD. As numerous as half of individuals with PD develop intellectual challenges, which can go from gentle carelessness to out and out dementia [46]. The dementia of PD is classified “subcortical” due to the area of influenced mind zones, and subcortical dementias have to some degree unexpected clinical side effects in comparison to a “cortical” dementia like AD. It affects the brain region orbitofrontal prefrontal cortex/ ventromedial cortex (OFC /VMPFC) and amygdala/hippocampus. The impedance of cognition in AD intently matches the deficiency of neural connections because of the poisonous impacts of A, tau, and aggravation [47]. Tau Protein is the main protein responsible for diseases which are neurogenerative. This pathology is characterized by tau accumulation in NFTs- neurofibrillary tangles.
In this present study, Potential associations within brain areas influenced by Alzheimer’s and Parkinson’s sick- ness is presented and examination about the relation between both the diseases is shown. It combines both imaging data, clinically relevant factors and previous research work related theories about the illness. As a result, considering how to delay or prevent the incidence of AD with respect to PD and vice-versa is obtained. The common affected brain areas are part of hippocampal volume frontal gyrus, paracingulate gyrus and the amyloid binding around anterior cingulate cortex (ACC).
Table 1. p value
|
Statistics: p-values adjusted for search volume |
|||||||||||||
|
Set-level |
Cluster-level |
Peak-level |
|
|
|
|
|||||||
|
p |
C |
pfWE-corr |
pfDR-corr |
kE |
puncorr |
pfWE-corr |
pfDR-corr |
T |
ZE |
puncorr |
mm |
mm |
mm |
|
0.000 |
10 |
NaN |
0.000 |
121345 |
0.000 |
0.000 |
0.000 |
33.71 |
Inf |
0.000 |
44 |
18 |
-10 |
|
|
|
|
|
|
|
0.000 |
0.000 |
29.28 |
Inf |
0.000 |
0 |
54 |
-8 |
|
|
|
|
|
|
|
0.000 |
0.000 |
29.23 |
Inf |
0.000 |
-2 |
56 |
4 |
|
|
|
0.000 |
0.000 |
10685.000 |
0.000 |
0.000 |
0.000 |
32.74 |
Inf |
0.000 |
18 |
-102 |
-54 |
|
|
|
|
|
|
|
0.000 |
0.000 |
30.78 |
Inf |
0.000 |
-28 |
-90 |
-62 |
|
|
|
|
|
|
|
0.000 |
0.000 |
28.53 |
Inf |
0.000 |
-18 |
-98 |
-58 |
|
|
|
0.000 |
0.000 |
113 |
0.000 |
0.000 |
0.000 |
8.57 |
7.04 |
0.000 |
-74 |
-2 |
-70 |
|
|
|
0.001 |
0.020 |
33 |
0.014 |
0.000 |
0.000 |
7.95 |
6.66 |
0.000 |
18 |
-42 |
-52 |
|
|
|
0.001 |
0.018 |
36 |
0.011 |
0.000 |
0.000 |
7.64 |
6.47 |
0.000 |
-18 |
-42 |
-52 |
|
|
|
0.000 |
0.000 |
104 |
0.000 |
0.000 |
0.000 |
7.08 |
6.11 |
0.000 |
72 |
40 |
-6 |
|
|
|
0.000 |
0.001 |
78 |
0.001 |
0.000 |
0.008 |
6.78 |
5.90 |
0.000 |
-2 |
-50 |
-46 |
|
|
|
|
|
|
|
0.016 |
0.327 |
5.73 |
5.16 |
0.000 |
-8 |
-56 |
-60 |
|
|
|
|
|
|
|
0.034 |
0.666 |
5.32 |
5.00 |
0.000 |
2 |
-60 |
-54 |
|
|
|
0.011 |
0.274 |
7 |
0.219 |
0.014 |
0.282 |
5.77 |
5.19 |
0.000 |
74 |
-74 |
28 |
|
|
|
0.021 |
0.422 |
3 |
0.422 |
0.015 |
0.290 |
5.77 |
5.18 |
0.000 |
78 |
-72 |
-8 |
|
|
|
0.018 |
0.391 |
4 |
0.352 |
0.017 |
0.334 |
5.72 |
5.15 |
0.000 |
-62 |
58 |
-14 |
[1] Noor, M.B.T., Zenia, N.Z., Kaiser, M.S., Mamun, S.A., Mahmud, M. (2020). Application of deep learning in detecting neurological disorders from magnetic resonance images: A survey on the detection of Alzheimer’s disease, Parkinson’s disease and schizophrenia. Brain Informatics, 7(1): 1-21. https://doi.org/10.1186/s40708-020-00112-2
[2] Ping, L., Duong, D.M., Yin, L., Gearing, M., Lah, J.J., Levey, A.I., Seyfried, N.T. (2018). Global quantitative analysis of the human brain proteome in Alzheimer’s and Parkinson’s Disease. Scientific Data, 5(1): 1-12. https://doi.org/10.1038/sdata.2018.36
[3] Ramig, L., Halpern, A., Spielman, J., Fox, C., Freeman, K. (2018). Speech treatment in Parkinson's disease: randomized controlled trial (RCT). Movement Disorders, 33(11): 1777-1791. https://doi.org/10.1002/mds.27460
[4] Van Bulck, M., Sierra-Magro, A., Alarcon-Gil, J., Perez-Castillo, A., Morales-Garcia, J.A. (2019). Novel approaches for the treatment of Alzheimer’s and Parkinson’s disease. International Journal of Molecular Sciences, 20(3): 719. https://doi.org/10.3390/ijms20030719
[5] Ellis, J.M., Fell, M.J. (2017). Current approaches to the treatment of Parkinson’s disease. Bioorganic & Medicinal Chemistry Letters, 27(18): 4247-4255. https://doi.org/10.1016/j.bmcl.2017.07.075
[6] DeTure, M.A., Dickson, D.W. (2019). The neuropathological diagnosis of Alzheimer’s disease. Molecular Neurodegeneration, 14(1): 1-18. https://doi.org/10.1186/s13024-019-0333-5
[7] Slot, R.E., Sikkes, S.A., Berkhof, J., Brodaty, H., Buckley, R., Cavedo, E., van der Flier, W.M. (2019). Subjective cognitive decline and rates of incident Alzheimer's disease and non-Alzheimer's disease dementia. Alzheimer's & Dementia, 15(3): 465-476. https://doi.org/10.1016/j.jalz.2018.10.003
[8] Lin, W., Tong, T., Gao, Q., Guo, D., Du, X., Yang, Y., Alzheimer’s Disease Neuroimaging Initiative. (2018). Convolutional neural networks-based MRI image analysis for the Alzheimer’s disease prediction from mild cognitive impairment. Frontiers in Neuroscience, 777. https://doi.org/10.3389/fnins.2018.00777
[9] Singleton, A., Hardy, J. (2016). The evolution of genetics: Alzheimer’s and Parkinson’s diseases. Neuron, 90(6): 1154-1163. https://doi.org/10.1016/j.neuron.2016.05.040
[10] Ball, N., Teo, W.P., Chandra, S., Chapman, J. (2019). Parkinson's disease and the environment. Frontiers in Neurology, 10: 218. https://doi.org/10.3389/fneur.2019.00218
[11] Hanagasi, H.A., Tufekcioglu, Z., Emre, M. (2017). Dementia in Parkinson's disease. Journal of the Neurological Sciences, 374: 26-31. https://doi.org/10.1016/j.jns.2017.01.012
[12] Raza, C., Anjum, R. (2019). Parkinson's disease: Mechanisms, translational models and management strategies. Life Sciences, 226: 77-90. https://doi.org/10.1016/j.lfs.2019.03.057
[13] Fiorenzato, E., Strafella, A.P., Kim, J., Schifano, R., Weis, L., Antonini, A., Biundo, R. (2019). Dynamic functional connectivity changes associated with dementia in Parkinson’s disease. Brain, 142(9): 2860-2872. https://doi.org/10.1093/brain/awz192
[14] Lott, I.T., Head, E. (2019). Dementia in Down syndrome: unique insights for Alzheimer disease research. Nature Reviews Neurology, 15(3): 135-147. https://doi.org/10.1038/s41582-018-0132-6
[15] Lanskey, J.H., McColgan, P., Schrag, A.E., Acosta-Cabronero, J., Rees, G., Morris, H.R., Weil, R.S. (2018). Can neuroimaging predict dementia in Parkinson’s disease? Brain, 141(9): 2545-2560. https://doi.org/10.1093/brain/awy211
[16] Ping, L., Duong, D.M., Yin, L., Gearing, M., Lah, J.J., Levey, A.I., Seyfried, N.T. (2018). Global quantitative analysis of the human brain proteome in Alzheimer’s and Parkinson’s Disease. Scientific Data, 5(1): 1-12. https://doi.org/10.1038/sdata.2018.36
[17] Shen, Y., Ye, B., Chen, P., Wang, Q., Fan, C., Shu, Y., Xiang, M. (2018). Cognitive decline, dementia, Alzheimer’s disease and presbycusis: examination of the possible molecular mechanism. Frontiers in Neuroscience, 12: 394. https://doi.org/10.3389/fnins.2018.00394
[18] Wang, L., Zang, Y., He, Y., Liang, M., Zhang, X., Tian, L., Li, K. (2006). Changes in hippocampal connectivity in the early stages of Alzheimer's disease: Evidence from resting state fMRI. Neuroimage, 31(2): 496-504. https://doi.org/10.1016/j.neuroimage.2005.12.033
[19] Rombouts, S.A., Barkhof, F., Goekoop, R., Stam, C.J., Scheltens, P. (2005). Altered resting state networks in mild cognitive impairment and mild Alzheimer's disease: An fMRI study. Human Brain Mapping, 26(4): 231-239. https://doi.org/10.1002/hbm.20160
[20] De Winter, F.L., Emsell, L., Bouckaert, F., Claes, L., Jain, S., Farrar, G., Vandenbulcke, M. (2017). No association of lower hippocampal volume with Alzheimer’s disease pathology in late-life depression. American Journal of Psychiatry, 174(3): 237-245. https://doi.org/10.1176/appi.ajp.2016.16030319
[21] Kumar, P.J., Yung, Y., Pan, M. (2020). Pragmatic realities on brain imaging techniques and image fusion for Alzheimer's disease. International Journal of Medical Engineering and Informatics, 12(1): 19-51.
[22] Espinoza, F.A., Anderson, N.E., Vergara, V.M., Harenski, C.L., Decety, J., Rachakonda, S., Kiehl, K.A. (2019). Resting-state fMRI dynamic functional network connectivity and associations with psychopathy traits. NeuroImage: Clinical, 24: 101970. https://doi.org/10.1016/j.nicl.2019.101970
[23] Johnson, K.A., Fox, N.C., Sperling, R.A., Klunk, W.E. (2012). Brain imaging in Alzheimer disease. Cold Spring Harbor Perspectives in Medicine, 2(4): a006213. https://doi.org/10.1101/cshperspect.a006213
[24] Sveinbjornsdottir, S. (2016). The clinical symptoms of Parkinson's disease. Journal of Neurochemistry, 139(s1): 318-324. https://doi.org/10.1111/jnc.13691
[25] Tysnes, O.B., Storstein, A. (2017). Epidemiology of Parkinson’s disease. Journal of Neural Transmission, 124(8): 901-905. https://doi.org/10.1007/s00702-017-1686-y
[26] Dwivedi, P., Chopra, J., Bhatia, M. (2021). Detecting depression in different stages of Alzheimer using PET imaging. 2021 11th International Conference on Cloud Computing, Data Science & Engineering (Confluence), pp. 487-493. https://doi.org/10.1109/Confluence51648.2021.9376887
[27] Garn, H., Coronel, C., Waser, M., Caravias, G., Ransmayr, G. (2017). Differential diagnosis between patients with probable Alzheimer’s disease, Parkinson’s disease dementia, or dementia with Lewy bodies and frontotemporal dementia, behavioral variant, using quantitative electroencephalographic features. Journal of Neural Transmission, 124(5): 569-581. https://doi.org/10.1007/s00702-017-1699-6
[28] McKetney, J., Runde, R.M., Hebert, A.S., Salamat, S., Roy, S., Coon, J.J. (2019). Proteomic atlas of the human brain in Alzheimer’s disease. Journal of Proteome Research, 18(3): 1380-1391. https://doi.org/10.1021/acs.jproteome.9b00004
[29] Higginbotham, L., Dammer, E.B., Duong, D.M., Modeste, E., Montine, T.J., Lah, J.J., Seyfried, N.T. (2019). Network analysis of a membrane-enriched brain proteome across stages of Alzheimer’s disease. Proteomes, 7(3): 30. https://doi.org/10.3390/proteomes7030030
[30] Adolfi, F., Couto, B., Richter, F., Decety, J., Lopez, J., Sigman, M., Ibáñez, A. (2017). Convergence of interoception, emotion, and social cognition: A twofold fMRI meta-analysis and lesion approach. Cortex, 88: 124-142. https://doi.org/10.1016/j.cortex.2016.12.019
[31] Guo, H., Zhang, Y. (2020). Resting state fMRI and improved deep learning algorithm for earlier detection of Alzheimer’s disease. IEEE Access, 8: 115383-115392. 10.1109/ACCESS.2020.3003424
[32] Bi, X.A., Jiang, Q., Sun, Q., Shu, Q., Liu, Y. (2018). Analysis of Alzheimer’s disease based on the random neural network cluster in fMRI. Frontiers in Neuroinformatics, 12: 60. https://doi.org/10.3389/fninf.2018.00060
[33] Hohenfeld, C., Nellessen, N., Dogan, I., Kuhn, H., Müller, C., Papa, F., Reetz, K. (2017). Cognitive improvement and brain changes after real-time functional MRI neurofeedback training in healthy elderly and prodromal Alzheimer’s disease. Frontiers in Neurology, 8: 384. https://doi.org/10.3389/fneur.2017.00384
[34] Wang, Z., Jia, X., Chen, H., Feng, T., Wang, H. (2018). Abnormal spontaneous brain activity in early Parkinson’s disease with mild cognitive impairment: A resting-state fMRI study. Frontiers in Physiology, 9: 1093. https://doi.org/10.3389/fphys.2018.01093
[35] Li, M., Liu, Y., Chen, H., Hu, G., Yu, S., Ruan, X., Xie, Y. (2019). Altered global synchronizations in patients with Parkinson’s disease: a resting-state fMRI study. Frontiers in Aging Neuroscience, 11: 139. https://doi.org/10.3389/fnagi.2019.00139
[36] Dujardin, K., Roman, D., Baille, G., Pins, D., Lefebvre, S., Delmaire, C., Jardri, R. (2020). What can we learn from fMRI capture of visual hallucinations in Parkinson’s disease. Brain Imaging and Behavior, 14(2): 329-335. https://doi.org/10.1007/s11682-019-00185-6
[37] Piramide, N., Agosta, F., Sarasso, E., Canu, E., Volontè, M.A., Filippi, M. (2020). Brain activity during lower limb movements in Parkinson’s disease patients with and without freezing of gait. Journal of Neurology, 267(4): 1116-1126. https://doi.org/10.1007/s00415-019-09687-1
[38] Dan, R., Růžička, F., Bezdicek, O., Roth, J., Růžička, E., Vymazal, J., Jech, R. (2019). Impact of dopamine and cognitive impairment on neural reactivity to facial emotion in Parkinson's disease. European Neuropsychopharmacology, 29(11): 1258-1272. https://doi.org/10.1016/j.euroneuro.2019.09.003
[39] Creese, B., Politis, M., Chaudhuri, K.R., Weintraub, D., Ballard, C., Aarsland, D. (2017). The psychosis spectrum in Parkinson disease. Nature Reviews Neurology, 13(2): 81-95. https://doi.org/10.1038/nrneurol.2016.200
[40] Lee, Y., Lee, S., Chang, S.C., Lee, J. (2019). Significant roles of neuroinflammation in Parkinson’s disease: therapeutic targets for PD prevention. Archives of Pharmacal Research, 42(5): 416-425. https://doi.org/10.1007/s12272-019-01133-0
[41] Kim, T., Vemuganti, R. (2017). Mechanisms of Parkinson’s disease-related proteins in mediating secondary brain damage after cerebral ischemia. Journal of Cerebral Blood Flow & Metabolism, 37(6): 1910-1926. https://doi.org/10.1177/0271678X17694186
[42] Zhang, X., Gao, F., Wang, D., Li, C., Fu, Y., He, W., Zhang, J. (2018). Tau pathology in Parkinson's disease. Frontiers in Neurology, 9: 809. https://doi.org/10.3389/fneur.2018.00809
[43] Guo, J.D., Zhao, X., Li, Y., Li, G.R., Liu, X.L. (2018). Damage to dopaminergic neurons by oxidative stress in Parkinson's disease. International Journal of Molecular Medicine, 41(4): 1817-1825. https://doi.org/10.3892/ijmm.2018.3406
[44] Caminiti, S.P., Presotto, L., Baroncini, D., Garibotto, V., Moresco, R.M., Gianolli, L., Perani, D. (2017). Axonal damage and loss of connectivity in nigrostriatal and mesolimbic dopamine pathways in early Parkinson's disease. NeuroImage: Clinical, 14: 734-740. https://doi.org/10.1016/j.nicl.2017.03.011
[45] Ganguly, G., Chakrabarti, S., Chatterjee, U., Saso, L. (2017). Proteinopathy, oxidative stress and mitochondrial dysfunction: Cross talk in Alzheimer’s disease and Parkinson’s disease. Drug Design, Development and Therapy, 11: 797-810. https://doi.org/10.2147/DDDT.S130514
[46] Colom-Cadena, M., Spires-Jones, T., Zetterberg, H., Blennow, K., Caggiano, A., DeKosky, S.T., Catalano, S.M. (2020). The clinical promise of biomarkers of synapse damage or loss in Alzheimer’s disease. Alzheimer's Research & Therapy, 12(1): 1-12. https://doi.org/10.1186/s13195-020-00588-4
[47] Tan, S.H., Karri, V., Tay, N.W.R., Chang, K.H., Ah, H.Y., Ng, P.Q., Candasamy, M. (2019). Emerging pathways to neurodegeneration: Dissecting the critical molecular mechanisms in Alzheimer’s disease, Parkinson’s disease. Biomedicine & Pharmacotherapy, 111: 765-777. https://doi.org/10.1016/j.biopha.2018.12.101