Zeynab Giyasova*![]() | Naila Eyvazova
| Naila Eyvazova![]() | Ilhama Mahmudova
| Ilhama Mahmudova![]() | Vusal Guliyev
| Vusal Guliyev![]() | László Vasa
| László Vasa![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
The safety and prosperity of a nation are intrinsically linked to the life expectancy of its population, given its role in capturing both the current health status and future prospects of its people. A healthy population is fundamental to national stability, economic development, and social cohesion. As such, identifying the determinants of life expectancy is essential for formulating policies that ensure the long-term security of the nation. This study provides the first empirical evidence of health expenditures’ causal effect on life expectancy in Kazakhstan. The linkage between health expenditures and life expectancy at birth in Kazakhstan is particularly pertinent, given the country's ongoing initiatives to enhance its healthcare infrastructure. With continued investments in health services, it is crucial to evaluate the connection between healthcare spending and life expectancy to determine the effectiveness of these financial commitments. This research utilizes the Toda-Yamamoto (T-Y) Granger causality test and Johansen cointegration analysis to explore the relationship between the variables for the period spanning 2000 to 2021. The results indicate that health expenditures significantly Granger-cause life expectancy, with a chi-square statistic of 9.497 and a p-value of 0.0021, signifying predictive power. Moreover, the Johansen cointegration analysis identifies a long-term equilibrium relationship between the both variables, highlighting the close interdependence between health outcomes and expected lifespan. These findings underscore the necessity for sustained investment in healthcare to enhance life expectancy. Policymakers in Kazakhstan should focus on the strategic allocation of healthcare resources to foster improved long-term health outcomes.
health, life expectancy, health expenditure, causality analysis, cointegration, public health safety, Kazakhstan
Health conditions and projected life expectancy are the key demographic metric components that encapsulate the overall health status, safety, and quality of life within a population. It reflects the estimated average lifespan of a newborn, assuming that existing age-specific mortality rates remain constant over the course of their life. As a composite indicator of human development, life expectancy is intricately linked to a nation's economic performance, social conditions, and the effectiveness of its healthcare system. It serves not only as a measure of individual well-being but also as a benchmark for evaluating public health policies and societal progress [1]. Mortality, defined as the process of generational extinction through individual deaths at different ages, directly influences life expectancy and serves as a critical metric for evaluating public health strategies [2]. Kazakhstan, the largest economy in Central Asia, has witnessed notable improvements in life expectancy over recent decades. In 2000, the average life expectancy at birth was 64.4 years, which increased by 5.92 years to reach 70.3 years in 2021 [3]. This positive trend coincides with various healthcare reforms and policy interventions aimed at enhancing medical services and public health infrastructure. The country’s population, currently estimated at 20.33 million in 2023, is projected to grow by 31% to 26.54 million by 2050, further underscoring the need for a robust healthcare system capable of supporting an aging demographic [3].
Kazakhstan's healthcare reforms have prioritized the decentralization of services to enhance rural healthcare access, the implementation of the family medicine model with integrated primary care teams, the promotion of preventive health measures and digital health solutions, and the strengthening of workforce capacity through targeted training initiatives. However, overall health expenditure continues to fall short of WHO benchmarks, prompting ongoing efforts to increase the share of primary healthcare funding to 60% of total health sector spending [4]. Health expenditures, which encompass financial resources allocated to preventive, curative, rehabilitative, and palliative care, play a crucial role in determining health outcomes. Investments in medical infrastructure, research, and public health initiatives contribute to improved healthcare accessibility and quality, ultimately impacting life expectancy [5]. Previous studies, such as the research by Chen and Goldman [6] have highlighted the interplay between healthcare financing, medical technology advancements, insurance coverage, and socioeconomic factors in shaping longevity. As global populations experience demographic shifts characterized by aging and rising prevalence of non-communicable diseases, the healthcare sector faces increasing demands that necessitate strategic investments [7]. In Kazakhstan, per capita health expenditures reached $403 in 2021, marking a 19.23% increase from the previous year [8]. However, despite rising healthcare spending, the effectiveness of these investments in extending life expectancy remains an open question.
Safety and health issues are paramount in industrial production and technology sectors, as they safeguard the well-being of workers and the environment. Effectively addressing these concerns through proper risk management and safety protocols is crucial for fostering a sustainable and livable world [9, 10]. The well-being and overall safety of a nation are often reflected in its life expectancy, particularly at birth, as it serves as a essential component of the overall health and development of a society. Improving life expectancy requires addressing various factors, including healthcare access, nutrition, sanitation, and social determinants of health, all of which play a vital role in establishing the foundation for national prosperity. The study explores the link between healthcare spending and life expectancy at birth in Kazakhstan, assessing how increased fiscal allocations may impact population longevity. By providing empirical insights into this dynamic, the study will inform policymakers on optimizing healthcare resource distribution to enhance public health outcomes.
A considerable body of literature has investigated the relationship between health expenditures and life expectancy, particularly in developing and transition economies. Several studies have found a positive impact of increased health spending on life expectancy, though the strength and characteristics of this relationship vary across different countries and regions.
Jaba et al. [11] examined the association between per capita healthcare expenditures and life expectancy at birth across 175 countries from 1995 to 2010 using panel data analysis. Their findings indicated a significant positive interrelation between healthcare spending and life expectancy, with variations observed across countries based on geographic location and income levels. Linden and Ray [12] investigated the relationship between life expectancy, public health expenditures, and private health expenditures in 34 OECD countries from 1970 to 2012 using panel time series methods. Their findings indicated a positive relationship between public health expenditures and life expectancy, with cointegration observed in countries with high public health spending. Furthermore, private health expenditures contributed to life expectancy but were affected by the level of public spending. Morina et al. [13] analyzed the impact of health expenditures and various socio-economic factors on life expectancy in OECD countries from 2005 to 2018 using multiple econometric models. Their findings confirmed a positive relationship between health expenditures and life expectancy, highlighting both the influence and causality of national longevity in these countries. Nkemgha et al. [14] conducted an empirical investigation into the relationship between health expenditures and life expectancy in Cameroon over the period 1980 to 2014. Employing Ordinary Least Squares (OLS) regression and the Toda-Yamamoto causality framework, the analysis revealed that private health expenditure has a statistically significant positive effect on life expectancy. In contrast, public health expenditure was not found to have a significant impact. Sango-Coker and Bein [15] examined healthcare spending in West Africa (1999–2014) using pooled regression and correlation analysis, finding a positive link between public health expenditure and life expectancy, but a negative association for private spending. These results suggest that increasing public healthcare expenditure would be more effective in improving life expectancy.
The relationship between health expenditures, life expectancy, economic growth, and environmental factors has been analyzed across various countries. Life expectancy, real GDP, and greenhouse gas emissions were found to significantly influence health expenditures, with life expectancy and GDP having a strong positive effect. Increases in government health expenditure, out-of-pocket payments, and external health expenditures were associated with improvements in life expectancy, emphasizing the critical role of financial investment in the healthcare sector [16, 17]. Polcyn et al. [18] investigated the influence of health expenditure, energy use, CO₂ emissions, population size, and income on health outcomes across 46 Asian countries between 1997 and 2019, employing advanced panel data methods. The study found that higher health expenditures and energy consumption contributed to improved health outcomes, while CO2 emissions negatively affected health. Healthcare spending emerged as the most influential factor in enhancing life expectancy, highlighting the need for increased investments in healthcare and CO2 reduction in Asian countries. Dorbonova and Sugözü [19] analyzed the long-run and causal interactions among health expenditures, renewable energy consumption, life expectancy, and GDP in Central Asian countries over the period 2000–2020, employing panel cointegration and Dumitrescu-Hurlin causality approaches. Their results indicated a significant bidirectional causal relationship between health expenditures and both renewable energy use and life expectancy, underscoring the importance of policy measures aimed at encouraging renewable energy investments to improve public health outcomes and support economic growth. Gulis et al. [20] examined the health status of Kazakhstan in relation to its political, economic, and social transitions since 1991, highlighting key trends such as a decline in life expectancy until 1996, followed by a recovery. Despite substantial investments in public health, the country continued to lag behind OECD nations on key health indicators, with cardiovascular diseases and child mortality remaining significant concerns. The authors identified seven strategic priorities aimed at improving the efficiency and effectiveness of the healthcare system. This research aims to fill the gap in understanding the causal relationship between health expenditures and life expectancy at birth in Kazakhstan through metric investigations. By analyzing this relationship, the study seeks to offer valuable insights into how health spending influences life expectancy within the context of Kazakhstan's evolving healthcare system.
This study investigates the impact of health expenditures on life expectancy in Kazakhstan utilizing annual time series data obtained from the World Bank [21]. The two key variables under analysis are Life Expectancy at Birth (LEAB) and Health Expenditures per Capita (HEPC). To reveal both the long-run equilibrium relationship and the causal dynamics between these variables, a combination of cointegration and causality tests is applied. This study is subject to limitations arising from the exclusion of relevant confounding variables that could also impact life expectancy, such as education, environmental conditions, and behavioral factors. Restricting the analysis to only HEPC and LEAB may inadequately represent the complex interplay of determinants influencing health outcomes. Future investigations should consider integrating a wider range of socioeconomic and ecological indicators to improve the analytical depth and reliability of the results.
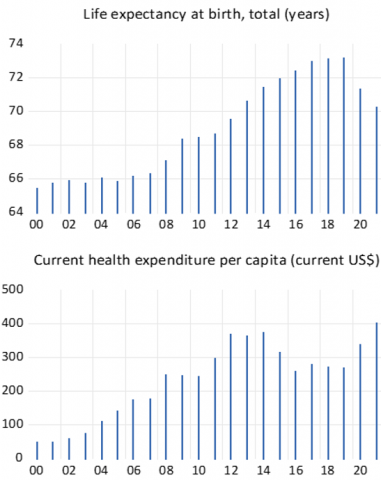
The bar charts presented in Figure 1 illustrate the temporal trends of life expectancy at birth and health expenditures per capita in Kazakhstan. The observed upward trajectory in both indicators suggests a potential positive correlation, implying that increased health expenditures may be contributing to improvements in life expectancy.
Figure 1. Trends in life expectancy at birth and health expenditures per capita in Kazakhstan (2000-2021)
Table 1. Descriptive analysis of data variables
|
Statistic |
LEAB |
HEPC |
|
Mean |
68.945 |
232.545 |
|
Median |
68.570 |
255.500 |
|
Maximum |
73.180 |
403.000 |
|
Minimum |
65.450 |
50.000 |
|
Std. Dev. |
2.826 |
112.304 |
|
Skewness |
0.186 |
-0.330 |
|
Kurtosis |
1.501 |
1.932 |
The data in Table 1 shows that HEPC in Kazakhstan display a significantly higher mean and standard deviation than LEAB, indicating greater variability in healthcare spending than in life expectancy. Additionally, the negative skewness observed in HEPC suggests a distribution with a longer tail towards lower health expenditure values, while the positive skewness in LEAB indicates a slight concentration of data points above the mean life expectancy.
The analytical process commences with an assessment of stationarity through unit root tests, such as the Augmented Dickey-Fuller (ADF) [22] test. If both variables exhibit stationarity at levels, the standard Vector Autoregressive (VAR) model is estimated. If one or both variables are non-stationary at levels but become stationary after first or second differencing, the Johansen cointegration test is applied within the VAR framework to assess the existence of a long-term equilibrium relationship between LEAB and HEPC. To evaluate short-run causal dynamics, the standard Granger causality [23] test is implemented within the VAR model. However, when variables are integrated at different orders, the Toda-Yamamoto Granger causality approach is utilized as a robust alternative. This method entails estimating an augmented VAR model by first determining the optimal lag length (K) using model selection criteria such as the Akaike Information Criterion (AIC) or Schwarz Information Criterion (SIC), followed by incorporating the maximum order of integration (Dmax) as additional lags to ensure the validity of statistical inferences.
The Toda-Yamamoto [24] procedure consists of several steps, with one of the initial tasks being the estimation of the VAR model using the optimal lag length, referred to as:
$Y_t=\sum_{i=1}^p A_i Y_{t-i}+\sum_{j=1}^{D_{\max }} B_j Y_{t-j}+\epsilon_t$ (1)
In this context, Yt represents a vector of the time series variables (such as LEAB and HEPC), Aidenotes the matrix of coefficients for the lags of the dependent variables, Bj refers to the matrix of coefficients for the augmented lags, and ϵt represents the error term. In addition to examining causal relationships, the study also employed the Johansen [25] cointegration method for analysis. The combination of these econometric methods allows for a comprehensive examination of both the long-term and short-term interactions between health expenditures and life expectancy, providing insights into the effectiveness of health-related investments in Kazakhstan.
Log transformations are applied in econometric modeling to simplify relationships, mitigate skewness, stabilize variance, and improve the interpretation of coefficients, especially when dealing with exponential growth or varying error variances.
Table 2 reveals that both LEAB and HEPC are non-stationary at levels and first differences but achieve stationarity upon second differencing, meaning Dmax is 2 and the variables are integrated of order of I(2). This suggests that these variables are shaped by long-term trends and structural factors, necessitating second differencing to remove non-stationary elements and enhance the robustness of econometric modeling.
Table 2. ADF unit root test
|
Variables |
Level |
1st Difference |
2nd Difference |
|
l_leap |
-1.443 (0.540) |
-1.704 (0.414) |
-5.419 (0.0004) |
|
l_hepc |
-2.184 (0.217) |
-2.941 (0.058) |
-6.040 (0.0001) |
Table 3 reports the results of the lag selection test for a time series model, where multiple information criteria (AIC, SC, HQ) consistently identify a lag of 1 as the optimal choice. This suggests that the current value of the time series is most effectively predicted by its preceding value. Additionally, the significant likelihood ratio (LR) statistic reinforces this selection, indicating that incorporating one lag significantly enhances the model fit compared to a specification without lags. Given that the number of endogenous variables (k) is 1, the model specification remains straightforward while ensuring robustness in capturing the underlying data dynamics.
Table 3. Optimal lag selection test
|
Lag |
LogL |
LR |
FPE |
AIC |
SC |
HQ |
|
0 |
27.262 |
NA |
0.000 |
-2.405 |
-2.306 |
-2.384 |
|
1 |
85.6416 |
100.0787* |
1.75e-06* |
-7.584* |
-7.286* |
-7.520* |
Note: * indicates the lag order selected by the criterion
Table 4 presents the roots of the characteristic polynomial for a VAR model comprising two endogenous variables, one exogenous variable (C), and lag specifications of 1 and 3. The fact that all roots have moduli less than 1 confirms the stability of the VAR model, implying that any shocks to the system will gradually dissipate, allowing the variables to revert to their long-run equilibrium.
Table 4. Roots of characteristic polynomial
|
Root |
Modulus |
|
0.837122 - 0.454799i |
0.952688 |
|
0.837122 + 0.454799i |
0.952688 |
|
0.905458 |
0.905458 |
|
-0.119972 - 0.555742i |
0.568544 |
|
-0.119972 + 0.555742i |
0.568544 |
|
-0.385281 |
0.385281 |
Table 5 presents the results of the Lagrange Multiplier (LM) test for serial correlation in the residuals of the Vector Autoregression (VAR) model across lags 1 to 4. The high p-values for both the LRE* and Rao F-statistics indicate that the null hypothesis of no serial correlation cannot be rejected at any lag. This confirms that the VAR residuals are free from serial correlation and can be regarded as white noise.
Table 5. VAR residual serial correlation LM tests
|
Lag |
LRE Stat |
df |
Prob. |
Rao F-stat |
df |
P-Value |
|
1 |
4.844 |
4 |
0.303 |
1.306 |
(4, 18.0) |
0.304 |
|
2 |
1.953 |
4 |
0.744 |
0.487 |
(4, 18.0) |
0.744 |
|
3 |
4.532 |
4 |
0.338 |
1.212 |
(4, 18.0) |
0.34 |
|
4 |
5.384 |
4 |
0.250 |
1.474 |
(4, 18.0) |
0.251 |
Table 6 presents the results of diagnostic tests for the residuals of a VAR model. The Jarque-Bera normality test indicates that the residuals, both individually and jointly, do not significantly depart from normality, as evidenced by the high p-values. Furthermore, the heteroskedasticity test provides no significant evidence of heteroskedasticity, with the high p-value suggesting that the variance of the residuals remains stable across observations. As a result, the residuals of the VAR model appear to fulfill the assumptions of normality and homoscedasticity.
Table 6. VAR residual normality and heteroskedasticity tests
|
Test |
Component/Chi-sq |
df |
P-Value |
|
Normality Test (Jarque-Bera) |
|
|
|
|
Component 1 |
2.168 |
2 |
0.338 |
|
Component 2 |
0.896 |
2 |
0.638 |
|
Joint |
3.064 |
4 |
0.547 |
|
Heteroskedasticity Test (Levels & Squares) |
|
|
|
|
Joint Test |
33.368 |
36 |
0.594 |
Table 7 reveals the findings of the Johansen cointegration tests and the T-Y Granger causality test. Both the trace and maximum eigenvalue tests suggest the existence of cointegration between the variables, as indicated by statistically significant p-values of 0.0018 and 0.0085 for the 'None' hypothesis, and 0.0190 for the 'At most 1' hypothesis in both tests. T-Y Granger causality test reveals that l_hepc significantly Granger-causes l_leap, with a chi-square statistic of 9.497, 3 degrees of freedom, and a p-value of 0.0021. This implies that past values of l_hepc provide valuable predictive information for future values of l_leap, beyond the predictive capacity of past values of l_leap alone.
Table 7. Johansen cointegration and Granger causality test results
|
Cointegration Rank Test - Trace |
|||
|
Hypothesized No of. CE(s) |
Eigenvalue |
Trace Statistic |
P-Value |
|
None |
0.650 |
24.421 |
0.0018 |
|
At most 1 |
0.263 |
5.504 |
0.0190 |
|
Cointegration Rank Test – Maximum Eigenvalue |
|||
|
Hypothesized No of. CE(s) |
Eigenvalue |
Max-Eigen Statistic |
P-Value |
|
None |
0.650 |
18.916 |
0.0085 |
|
At most 1 |
0.263 |
5.504 |
0.0190 |
|
Causality Test – l_hepc to l_leap |
|||
|
Chi-square |
df |
k |
P-Value |
|
9.497 |
3 |
1 |
0.0021 |
This study employed the Toda-Yamamoto approach, which revealed that health expenditures significantly Granger-cause life expectancy in Kazakhstan, indicating that past changes in health spending can predict future life expectancy. The Johansen cointegration test confirmed a long-term equilibrium relationship among the variables, with evidence of at least one cointegrating vector. These results suggest potential long-term benefits of increased healthcare investment, while highlighting the need for further research to clarify mechanisms and guide health policy in Kazakhstan. A number of other studies have yielded similar results using the Johansen cointegration and Granger causality test methods, further strengthening the established relationship between health expenditures and life expectancy [26, 27]. These studies underscore the significance of causality in analyzing how fluctuations in health spending can influence life expectancy across various regional or contextual frameworks. Although the empirical findings establish a significant long-term association and causal relationship between health expenditures and life expectancy in Kazakhstan, a deeper exploration of the mechanisms underlying this link is necessary. Elevated health spending can facilitate improved access to healthcare services, enhance the quality of medical care, and strengthen preventive and public health initiatives, collectively contributing to lower mortality rates and increased longevity [28]. Furthermore, investments in healthcare infrastructure and the development of human resources in the medical sector enable earlier detection and more effective management of chronic conditions, thereby promoting extended and healthier lifespans.
The health and longevity of a nation's population are fundamental to its overall safety, stability, and long-term prospects. Life expectancy is a crucial indicator of public health, reflecting not only the present health outcomes but also the success of government policies and healthcare investments. In Kazakhstan, where considerable resources are being allocated to enhance the healthcare sector, it is essential to understand the connection between health expenditures and life expectancy in order to evaluate the effectiveness of these investments. As Kazakhstan continues to expand and modernize its healthcare infrastructure, evaluating the influence of health expenditures on life expectancy remains a vital area of inquiry. This study provides compelling evidence of a significant association between healthcare spending and life expectancy within the country. The application of the Johansen cointegration test confirms the presence of a long-term equilibrium relationship between these variables, suggesting that sustained investment in healthcare may yield enduring improvements in population health. Specifically, the trace statistic for the 'None' hypothesis is 29.451 with a p-value of 0.0018, and the maximum eigenvalue statistic for the same hypothesis is 22.375 with a p-value of 0.0085, confirming the presence of at least one cointegrating vector. The 'At most 1' hypothesis is also supported, with a p-value of 0.0190, suggesting a stable long-term association. In addition, the T-H Granger causality test shows that health expenditures significantly Granger-cause life expectancy, with a chi-square statistic of 9.497 and a p-value of 0.0021. This finding indicates that past variations in health spending can predict future life expectancy, highlighting the importance of continued investment in healthcare. These results emphasize the need for efficient allocation of healthcare spending to maximize improvements in life expectancy and public health outcomes in Kazakhstan. Policy recommendations include prioritizing increased investment in primary and preventive healthcare, upgrading medical infrastructure and digital health technologies, enhancing healthcare workforce training and capacity, and establishing robust monitoring and evaluation systems to improve the efficiency and impact of health spending in Kazakhstan.
[1] Bilas, V., Franc, S., Bošnjak, M. (2014). Determinant factors of life expectancy at birth in the European Union countries. Collegium Antropologicum, 38(1): 1-9.
[2] Bureau of National Statistics. (2024). Life expectancy at birth of the population of the Republic of Kazakhstan. Bureau of National statistics. Agency for Strategic planning and reforms of the Republic of Kazakhstan. https://stat.gov.kz/en/industries/social-statistics/demography/publications/157663/.
[3] WHO Data. (2024). Kazakhstan. Health data overview for the Republic of Kazakhstan. https://data.who.int/countries/398.
[4] Qumar, A.B., Kulzhanov, M., Kosherbayeva, L. (2024). Primary healthcare reform in Kazakhstan: A socially-oriented model. Central Asian Journal of Medical Hypotheses and Ethics, 5(4): 250-258. https://doi.org/10.47316/cajmhe.2024.5.4.01
[5] Edejer, T.T.T., Garg, C., Hernandez, P., Van De Maele, N., Indikadahena, C. (2008). Health care costs, structures and trends. International Encyclopedia of Public Health, pp. 153-160. https://doi.org/10.1016/B978-012373960-5.00163-5
[6] Chen, A., Goldman, D. (2016). Health care spending: Historical trends and new directions. Annual Review of Economics, 8(1): 291-319. https://doi.org/10.1146/annurev-economics-080315-015317
[7] Yeganeh, H. (2019). An analysis of emerging trends and transformations in global healthcare. International Journal of Health Governance, 24(2): 169-180. https://doi.org/10.1108/IJHG-02-2019-0012
[8] Macrotrends. (2025). Kazakhstan Healthcare Spending. https://www.macrotrends.net/global-metrics/countries/KAZ/kazakhstan/healthcare-spending#:~:text=Current%20expenditures%20on%20health%20per,a%2019.23%25%20increase%20from%202020.
[9] Hasanov, R.I., Giyasova, Z., Musayeva, R., Zemri, B.E., Kazimova, A. (2024). Examining the relationship between primary aluminium production and accident rates. International Journal of Safety and Security Engineering, 14(5): 1403-1408. https://doi.org/10.18280/ijsse.140507
[10] Hasanov, R.I. (2023). Towards a sustainable future in aluminium production: Environmental and economic benefits of revolutionary inert anode technology. Journal of Sustainability Science and Management, 18(10): 176-186. http://doi.org/10.46754/jssm.2023.10.012
[11] Jaba, E., Balan, C.B., Robu, I.B. (2014). The relationship between life expectancy at birth and health expenditures estimated by a cross-country and time-series analysis. Procedia Economics and Finance, 15: 108-114. https://doi.org/10.1016/S2212-5671(14)00454-7
[12] Linden, M., Ray, D. (2017). Life expectancy effects of public and private health expenditures in OECD countries 1970–2012: Panel time series approach. Economic Analysis and Policy, 56: 101-113. https://doi.org/10.1016/j.eap.2017.06.005
[13] Morina, F., Komoni, A., Kilaj, D., Selmonaj, D., Grima, S. (2022). The effect of health expenditure on life expectancy. International Journal of Sustainable Development and Planning, 17(5): 1389-1401. https://doi.org/10.18280/ijsdp.170502
[14] Nkemgha, G.Z., Tékam, H.O., Belek, A. (2021). Healthcare expenditure and life expectancy in Cameroon. Journal of Public Health, 29: 683-691. https://doi.org/10.1007/s10389-019-01181-2
[15] Sango-Coker, E.Y., Bein, M.A. (2018). The impact of healthcare spending on life expectancy: Evidence from selected West African countries. African Journal of Reproductive Health, 22(4): 64-71.
[16] Bayar, Y., Gavriletea, M.D., Pintea, M.O., Sechel, I.C. (2021). Impact of environment, life expectancy and real GDP per capita on health expenditures: Evidence from the EU member states. International Journal of Environmental Research and Public Health, 18(24): 13176. https://doi.org/10.3390/ijerph182413176
[17] Owumi, B.E., Eboh, A. (2021). An assessment of the contribution of healthcare expenditure to life expectancy at birth in Nigeria. Journal of Public Health, 30: 2113-2121. https://doi.org/10.1007/s10389-021-01546-6
[18] Polcyn, J., Voumik, L.C., Ridwan, M., Ray, S., Vovk, V. (2023). Evaluating the influences of health expenditure, energy consumption, and environmental pollution on life expectancy in Asia. International Journal of Environmental Research and Public Health, 20(5): 4000. https://doi.org/10.3390/ijerph20054000
[19] Dorbonova, İ., Sugözü, İ.H. (2024). Analyzing the relationship between health expenditure, renewable energy and life expectancy: Evidence from Asian countries. ESAM Ekonomik ve Sosyal Araştırmalar Dergisi, 5(1): 111-134. https://doi.org/10.53662/esamdergisi.1459607
[20] Gulis, G., Aringazina, A., Sangilbayeva, Z., Kalel, Z., de Leeuw, E., Allegrante, J.P. (2021). Population health status of the Republic of Kazakhstan: Trends and implications for public health policy. International Journal of Environmental Research and Public Health, 18(22): 12235. https://doi.org/10.3390/ijerph182212235
[21] World Bank Group. (2024). Data: Kazakhstan. https://data.worldbank.org/country/kazakhstan?view=chart.
[22] Dickey, D.A., Fuller, W.A. (1979). Distribution of the estimators for autoregressive time series with a unit root. Journal of the American Statistical Association, 74(366a): 427-431. https://doi.org/10.1080/01621459.1979.10482531
[23] Granger, C.W.J. (1969). Investigating causal relations by econometric models and cross-spectral methods. Econometrica: Journal of the Econometric Society, 37(3): 424-438. https://doi.org/10.2307/1912791
[24] Toda, H.Y., Yamamoto, T. (1995). Statistical inference in vector autoregressions with possibly integrated processes. Journal of Econometrics, 66(1-2): 225-250. https://doi.org/10.1016/0304-4076(94)01616-8
[25] Johansen, S. (1988). Statistical analysis of cointegration vectors. Journal of Economic Dynamics and Control, 12(2-3): 231-254. https://doi.org/10.1016/0165-1889(88)90041-3
[26] Liu, H., Zhong, K. (2022). Relationship between health spending, life expectancy and renewable energy in China: A new evidence from the VECM approach. Frontiers in Public Health, 10: 993546. https://doi.org/10.3389/fpubh.2022.993546
[27] Ye, L., Zhang, X. (2018). Nonlinear granger causality between health care expenditure and economic growth in the OECD and major developing countries. International Journal of Environmental Research and Public Health, 15(9): 1953. https://doi.org/10.3390/ijerph15091953
[28] World Health Organization. (2010). Health systems financing: The path to universal coverage. World Health Report 2010. https://www.who.int/publications/i/item/9789241564021.