A A I N Marhaeni*![]() | I Ketut Sudibia
| I Ketut Sudibia![]() | Dewa Jati Primajana T | I A Laksmi | Diah Pradnyadewi | Made Santana Putra Adiyadnya | Gede Andika
| Dewa Jati Primajana T | I A Laksmi | Diah Pradnyadewi | Made Santana Putra Adiyadnya | Gede Andika ![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
The success of the Family Planning Program, which has been implemented for almost 53 years in Bali Province, has changed the age structure of the population into an aging population structure, where the proportion of the elderly population (aged 60 + years) is now above 10 percent. All regencies experience the same situation, including in Karangasem Regency, where in 2020, based on the results of the Population Census, the percentage of elderly reached 13.07 percent. The significant decline in births in Bali Province as well as in Karangasem Regency has resulted in the average number of children per family decreasing to 2.31 children per family in 2020. The decreasing number of children and the increasing proportion of the elderly, along with the rising life expectancy, have had an impact on elderly care. Elderly people in their lives may live alone or only with their spouse, which becomes problematic as they age. In such conditions, it is hoped that the government will step in to address this issue. The purpose of this research is to design appropriate policy scenario models in handling elderly people, whether poor or non-poor, who live alone or only with their spouse. Another objective is to identify the parties most influential in determining the quality of life for the elderly. Data were collected through focus group discussions (FGDs) with participants including various parties involved in elderly care such as families, district governments, and village governments. The data analysis techniques used are multi-policy analysis and Mactor Analysis, which include sustainability analysis. The research results show that elderly individuals living alone or only with their spouse, whether classified as poor or non-poor, have the following policy priorities for their care: 1) The top priority policy is the construction of special housing for the elderly at the village level; 2) The second priority is the policy of providing elderly care in their own homes; and 3) The last priority policy is the placement of the elderly in existing nursing homes/elderly care facilities. These policies should be funded through collaborative efforts between village governments, related agencies, and private foundations. The parties most influential in improving the quality of life for the elderly are children and the Health Department (health workers), who exhibit the strongest convergence. Suggestions that can be put forward are the need for commitment from the relevant parties, especially village governments, district and provincial governments, and elderly care advocates, to handle elderly issues at the village level by building simple but elderly-friendly homes at the village level, specifically for elderly individuals living alone or only with their spouse who already require assistance in their daily lives.
elderly, alone, home, friendly, poor
Population issues faced by each country differ over time. The challenges from 50 years ago, for instance, are distinct from those faced today. This is evident in Indonesia, as well as at the provincial and district levels, where demographic issues have evolved over time. The Family Planning Program in Indonesia and Bali Province, implemented more than 50 years ago, has significantly impacted family sizes. Previously, the average number of children born per family in Indonesia and Bali was nearly six, but it has now decreased to around two. Similar conditions have also been observed in other countries, such as Brazil [1]. Economic and health advancements have contributed to increased life expectancy, allowing people to live longer. As a result, the proportion of the elderly population is increasing in many regions, including Bali Province and Karangasem Regency. Population aging is a global phenomenon that is becoming increasingly urgent in developing countries [2]. One key indicator of health policy is the average life expectancy, which tends to rise over time. This trend is accompanied by accelerated population aging and an increased proportion of elderly individuals within the population structure [3]. Similar trends of rising elderly proportions are seen in countries like Brazil and South Korea [1, 3-5]. Various studies predict that by 2050, the global population aged 60 + years will double [6]. This increase in the elderly population, both in absolute numbers and proportion, is occurring in nearly every country worldwide. Aging typically affects the quality of life of the elderly [7].
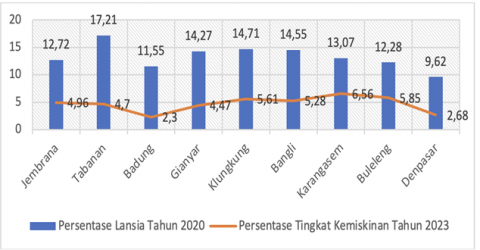
Figure 1. Percentage of elderly population based on the 2020 population census data and percentage of poverty levels in regencies/cities of Bali Province in 2023
The data in Figure 1 show that the elderly population, particularly those aged 60 + years, continues to increase and varies across regencies/cities in Bali Province. Similarly, the percentage of the poor population varies between regencies/cities. Figure 1 also indicates that all regions need to address elderly residents, especially those who are economically disadvantaged or living alone or with only their spouse.
Addressing elderly individuals in low-income or impoverished groups is also part of implementing sustainable development as per the Sustainable Development Goals (SDGs), which Indonesia has ratified. There are 17 SDGs, of which three are related to reducing poverty, ending hunger, and ensuring good health and well-being, which are the first, second, and third goals, respectively. Reducing poverty and hunger, along with promoting good health and well-being, are considered critical goals to be achieved by countries that ratified the SDGs in 2014, to support national development, including increasing public welfare. The reduction of poverty and hunger, which is a key goal, is also in line with Bappenas’ priority targets on social development, focusing on several objectives, including no poverty, no hunger, good health and well-being, quality education, and gender equality [8]. This social development is aligned with the SDGs, so the success of social development will also ensure the success of sustainable development.
Addressing elderly individuals, especially from low-income families who live alone or with only their spouse, is very important as it is related to the SDGs and national development goals, especially in implementing Article 34 of the 1945 Constitution. Therefore, designing or discovering ideal policies for elderly care becomes very important to develop practical policies for elderly individuals who require significant attention from various parties, especially the government, which has the largest responsibility for improving public welfare [9]. To achieve this goal, this research is urgently needed to scientifically design or discover ideal elderly care models, especially for the economically disadvantaged elderly who live alone or with only their spouse. Additionally, to enrich the discussion and deepen the information on elderly care, the study will also examine the care models that elderly individuals, who still live with their families, expect. Many elderly individuals feel unappreciated and lonely, which can lead to stress [10]. Research in rural Nepal has also shown abuse and neglect of elderly individuals by their families [11].
This study is not aimed at elderly individuals cared for by their children, as they do not have significant issues. This study focuses on elderly individuals living alone or with only their spouse, without other family members, which raises concerns about their welfare [12]. Over time, elderly individuals will increasingly need assistance from others. The question arises: who should be responsible for their care, the central government, provincial government, district government, or village government?
At the district level, the social service department employs Social Welfare Workers at Tenaga Kesejahteraan Sosial Kecamatan (TKSK), who are responsible for assisting or visiting elderly individuals in their homes. However, there is only one TKSK officer per subdistrict, covering a relatively large area. As a result, daily visits to elderly individuals, especially those living alone or with only their spouse, are not possible due to the limited number of workers. Many elderly individuals in the research area are also unwilling to leave their villages to live elsewhere, as they prefer to stay in their local communities. However, as they age, they become more dependent on their environment, which may require daily visits from the TKSK officers, something that cannot be done due to the limited number of workers.
Given these circumstances, solutions are needed for the care of elderly individuals in such conditions. Therefore, the purpose of this research is to: 1) design an ideal care model for elderly individuals in low-income groups living alone or with only their spouse; 2) design an ideal care model for elderly individuals in non-poor families living alone or with only their spouse; 3) identify the parties involved in determining the quality of life for elderly individuals in Karangasem District. Based on these research goals, the findings will provide input to relevant parties, including governments at the provincial, district, and village levels, as well as other stakeholders, to develop care models for elderly individuals in such conditions. In addition, the findings can serve as a basis for expanding the participation of various parties in elderly care, thus improving the quality of life for elderly individuals.
Indonesia has an aging demographic structure, with the percentage of people aged 65 and above predicted to increase by 25 percent, or around 80 million, by 2050. This increase in the elderly population will raise the dependency ratio, as the elderly are highly vulnerable to becoming dependent on younger family members who live with them. This situation also exacerbates the conditions experienced by the productive-age population, as they must support unproductive family members, limiting their self-investment and increasing household consumption burdens. The situation for elderly individuals who are unproductive worsens if they live in poverty and alone or without relatives. During the COVID-19 pandemic, the welfare of the elderly became a particular focus for the government. Research by Handayani [13] shows that elderly individuals who were able to work before the pandemic became unable to work afterward, becoming dependent on family members due to their inability to work and lack of a pension. One program provided to the elderly is through Program Keluarga Harapan (PKH). Findings by Ramadhan and Hidir [14] indicate that elderly individuals significantly benefit from PKH for daily and health needs. The implementation of PKH has also followed procedures, delivering maximum impact for elderly individuals from low-income families [15]. Other assistance programs contributing to the welfare of the elderly and effectively improving their quality of life include the BPJS Kesehatan program, BPNT, and PKH.
Research by Maifizar [16] on the poverty phenomenon in poor rural families in Aceh shows that poverty also affects the elderly without productive family members. These elderly individuals face welfare issues, as they must work at an advanced age to earn income, often with limited transportation access and long distances to resources such as rivers to meet their needs. Parwodiwiyono [17] also states that a significant portion of the elderly population lives in poverty, with findings showing that 17.2 percent of the elderly population in D.I Yogyakarta lives in poverty. Research on elderly individuals in Subokerto Village, Boyolali, found a link between elderly depression levels and their social interactions in the community [18]. This relationship is negative, meaning that the higher the level of depression, the lower the social interaction, and vice versa. Based on these findings, reducing elderly depression levels is crucial for improving their social interactions and, consequently, their welfare. Other studies examining the relationship between social support and the quality of life of the elderly suggest that higher social support, which includes having relatives, trustworthy people, caring individuals, and loving family members, significantly affects the quality of life for the elderly [19]. This research highlights the importance of family support in enhancing the quality of life for the elderly. Other findings also show that social support positively correlates with the happiness of the elderly. No significant differences were found in the happiness levels of elderly individuals in Mekarsari Village and those at PSTW “Budhi Dharma” in Bekasi. Social support significantly and positively impacts the happiness of the elderly [20]. Communication, Information, and Education (KIE) or empowerment about their health is crucial for improving the quality of life for the elderly. Elderly individuals participating in empowerment programs have higher average quality of life and health behavior scores [21]. During the COVID-19 pandemic, many elderly individuals were forced to stay home, facing social support issues and worsening physical and mental health, which could even increase family conflicts [22, 23].
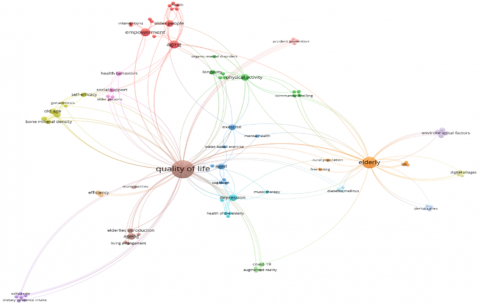
Research on the conditions of non-productive elderly individuals and assistance programs that help maintain their consumption has been widely discussed in empirical studies, such as the elderly's dependence on younger age groups, household burdens, and the effectiveness of government programs for supporting elderly individuals in such conditions. However, limited research has explored elderly individuals in poor families who have no relatives or family members to assist them. Therefore, this study will analyze the conditions of poor elderly individuals without relatives using primary data analyzed statistically and through multi-policy techniques. Furthermore, this study will use Mactor Analysis techniques to examine the stakeholders involved in improving the quality of life for the elderly. This study differs from previous research by focusing on ideal caregiving models for elderly individuals who live alone or only with their spouse. Below is an image showing the bibliometric visualization network of published articles on the quality of life.
Figure 2 shows the diversity of themes studied concerning the quality of life of the elderly. Additionally, themes on empowerment, particularly elderly empowerment, are frequently explored. Various aspects related to elderly health and the types of illnesses and contributing factors are also commonly studied. Elderly-friendly housing is an important aspect examined in this study, which has rarely or not been discussed.
Figure 2. Bibliometric visualization network using VOSviewer
The approach used in this research is a qualitative or exploratory design, as various elements of the analysis are based on results from exploratory field activities. A sustainability analysis using multi-policy data analysis techniques is employed in this study. The data analyzed using this technique is obtained from focus group discussions (FGDs) involving various stakeholders, such as village heads, TKSK (social welfare workers) across Karangasem Regency, the Social Services Office of Karangasem Regency, children of elderly individuals who care for their parents, academics, and community leaders. In addition to FGDs, data collection methods also include in-depth interviews with various related parties, including elderly individuals living alone or only with their spouse, whether poor or not. The results of these interviews are used to create a more in-depth discussion. Data from the FGDs is used for analysis through the sustainability analysis technique, particularly multi-policy analysis. There are three main elements in multi-policy analysis: scenarios, policies, and actions or programs [24]. The weights for these main elements are assigned as follows: scenarios are weighted from 1–6, policies from 0–100, and actions from 0–100. The weights for these three main elements are determined through FGDs. Based on the FGDs conducted, the weights of each element and the indicators for each element are outlined as follows and will serve as input factors for multi-policy analysis.
The information in Table 1 shows the presence of 2 scenarios, 5 criteria, 3 policies, and 6 actions. After obtaining the information in Table 1, the filling out of the 3 required matrices: 1) the Matrix of Actions against Criteria, 2) the Matrix of Policy against Criteria, and 3) the Matrix of Scenario against Criteria, is also based on the results of FGDs. These three matrices serve as the data used in the multi-policy analysis [24, 25]. To address the third objective of the research, the Mactor sustainability analysis technique is also utilized to identify the parties involved in determining the quality of life for the elderly. Furthermore, the Mactor Analysis can be used as a reference for formulating various proposed policies [24, 26, 27].
Table 1. Scenarios, criteria, policies, and actions in the care model for poor and non-poor populations living alone or with their spouse
|
A |
Scenario |
Code |
Weight |
|
1 |
Model of caring for poor elderly people who live alone/together with their partner |
POOREL |
6 |
|
2 |
Model of caring for non-poor elderly people who live alone/together with their partner |
NONPOOREL |
5 |
|
B |
Criteria |
Code |
Weight |
|
1 |
Availability of safe homes for the elderly people |
SAFEHOME |
6 |
|
2 |
Increasing the life expectancy of the elderly people |
LIFEEXPECT |
4 |
|
3 |
Focused social assistance from the community |
FOCUSED |
3 |
|
4 |
Increased certainty for caring of elderly people |
CERTAINTY |
5 |
|
5 |
Increased availability of village public facilities for the community |
VILLAGEPUB |
4 |
|
C |
Policy |
Code |
Weight |
|
1 |
Construction of special houses for the elderly at the village level |
SPECIALHOUS |
6 |
|
2 |
Placement of the elderly in existing nursing homes |
NURSINGHOM |
4 |
|
3 |
Elderly care at their each home |
THEIRHOM |
5 |
|
D |
Action |
Code |
|
|
1 |
Funding for handling the elderly collaborates between the village government, related agencies and private foundations |
COLLABORATES |
|
|
2 |
Construction of housing facilities and facilities using state/village land |
FACILITIES |
|
|
3 |
Providing motivation to the elderly to be willing to live elsewhere (Panti or other place) |
MOTIVATION |
|
|
4 |
Placement in the orphanage/place closest to the village and in the same place |
ORPHANAGE |
|
|
5 |
Providing assistance in the form of money, basic needs and periodic health checks by the village/relevant agency |
MONEYAND |
|
|
6
|
Periodic visits by villages/relevant agencies
|
VISITS
|
|
4.1 Ideal care/management model for elderly individuals in poor or non-poor families living alone or only with their spouse
To develop an ideal care/management model for elderly individuals living alone or only with their spouse, whether poor or non-poor, the prospective analysis technique or multi-policy sustainability analysis was employed. This analysis technique follows the sequence of analysis outlined below.
4.1.1 Evaluation of the interrelationship between policies and programs
This matrix comprises the scores of programs/actions related to policies. It also includes the average/mean values, standard deviations, and rankings of programs/actions based on policies named "Number" in the multi-policy framework. The higher the rank or "Number" value, the better the performance of the program/action, and vice versa. Based on the output of the multi-policy analysis, the interrelationship between policies and programs is presented in the following matrix.
In Table 2, there are several explanations, namely, the symbol Moy represents the average/mean score, Ec. Ty indicates the standard deviation, and Number represents the ranking of the program/actions based on the policy. The first multi-policy analysis results in Table 2 show that the highest-ranking program, indicated by the Number with the highest value, which is 6, is the COLLABORAT program, which is a Funding Program for elderly care in collaboration between the village government, related agencies, and private foundations. Thus, the program with the highest score is related to funding, followed by the FACILITIES program, which focuses on the development of housing facilities and infrastructure using state/village land, and similarly, the other values. The lowest Number value is VISIT, which is a periodic visit by the village/related agency. The visits refer to visiting elderly people periodically at their homes, which can be carried out by the village/related agency. Types of health services that can be provided to the elderly include daily living activities testing, mental status testing, weight measurement, and height measurement to obtain body mass index. This also includes nutritional status testing, blood pressure measurement, hemoglobin testing, blood sugar testing for early detection of diabetes, urinary protein testing for early detection of kidney disease, referrals to the local health center if abnormalities are found, health consultations and advice, home visits by executives, provision of supplementary food, and exercise activities [28]. The VISIT program has the lowest score because the workforce for visiting elderly homes/special elderly homes at the village level is very limited. Even the distance between one elderly home and another is very far, and some are on hills, so reaching them takes a long time. In other words, the resources required, especially human resources, to carry out this program are very large. Therefore, visits, if conducted to one location (e.g., a special elderly home in the village or in a nursing home), will require only a one-time effort but will meet many elderly people, compared to if the elderly remain in their individual homes.
In addition to using the data, the relationship between the program (actions) and policy can also be depicted in a Profile Map in a visual form to observe both variables. The Profile Map of the relationship between the program (actions) and policy is presented in Figure 3.
The COLLABORAT program (funding program for elderly care in collaboration with village governments, related agencies, and private foundations) and FACILITIES program (construction of housing facilities using state/village land) are the most effective in the SPECIALHOUS policy (policy for building special homes for the elderly at the village level). This can be understood because, in the policy of building special homes for the elderly at the village level, funding programs in collaboration with village governments, related agencies, and private foundations are essential. Similarly, in the policy of building special homes for the elderly at the village level, there is a need for programs to develop facilities and housing infrastructure using state/village land. Several studies indicate that because hospitals and clinics providing professional medical services are concentrated in urban areas [29-31], rural communities tend to have less access to healthcare services compared to those living in urban areas, especially for communities in geographically difficult-to-reach areas by public transportation. In the NURSINGHOM policy (policy for placing the elderly in existing nursing homes), funding programs for elderly care in collaboration with village governments, related agencies, and private foundations are also needed to improve the management of nursing homes.
Table 2. Matrix of policy-program interrelations (policies and actions)
|
|
SPECIALHOU |
NURSINGHOM |
THEIRHOM |
Moy. |
Ec. Ty |
Number |
|
COLLABORAT |
15.5 |
12.2 |
13.8 |
14.1 |
1.3 |
6 |
|
FACILITIES |
15 |
13 |
13 |
13.8 |
1 |
5 |
|
MOTIVATION |
9.9 |
12.1 |
11.1 |
10.9 |
0.9 |
2 |
|
ORPHANAGE |
12.4 |
11.9 |
11.6 |
12 |
0.4 |
4 |
|
MONEYAND |
11.3 |
11.3 |
11.9 |
11.5 |
0.3 |
3 |
|
VISITS
|
8.7
|
8.4
|
9.8
|
9
|
0.6
|
1
|
Figure 3. Profile Map of the care model for poor and non-poor elderly
Figure 4. Proximity map of policy and program/actions interrelationships
According to Tamher and Noorkasiani [32], one of the government's social efforts to improve the welfare of the elderly is by establishing social organizations or nursing homes. Nursing homes (Panti Tresna Werdha) are institutions where elderly people who are physically and mentally still independent live, and their daily needs are usually provided by the management [33]. In the THEIRHOM policy (policy for elderly care at their own homes), funding programs for the elderly in collaboration with village governments, related agencies, and private foundations are also needed to provide assistance to the elderly, especially those who are poor.
To visualize the proximity between policies and actions/programs, the multi-policy analysis presents the results in the form of a map, as shown in Figure 4.
Figure 4 clearly shows the correlation between policies and the corresponding or closely related programs/actions. In the SPECIALHOU Policy (Development of special homes for the elderly at the village level), 2 programs/actions are closely related or appropriate: 1) The funding program for elderly care in collaboration with the village government, related agencies, and private foundations; 2) The program for building facilities and housing infrastructure by utilizing state/village land. With these 2 programs/actions, the policy of developing special homes for the elderly at the village level can be realized. On the other hand, in the NURSINGHOM Policy (Placement of the elderly in existing nursing homes), there are 2 programs/actions that are closely related or suitable: 1) The program to motivate the elderly to be willing to live in other places (such as nursing homes or other facilities); 2) The program to place the elderly in the nearest nursing home within the same location. Many elderly people prefer to live in their own homes rather than in nursing homes [34]. Adib [35] stated that the elderly prefer to stay at home or with family, so the program to motivate them to relocate becomes essential. Additionally, placing the elderly in nursing homes close to the village and ensuring those from the same village are placed in the same facility is also a program that can be implemented to increase the elderly's willingness to move. Hurlock [36] mentions that several factors affect the elderly's choice of living arrangements, including economic status, marital status, health, ease of care, gender, children, desire for companionship, and climate. In the THEIRHOM Policy (Elderly Care at Their Own Homes), there are also 2 programs/actions that are closely related or suitable: 1) Periodic visits by the village/related agencies; 2) Provision of assistance in the form of money, basic necessities, and periodic health checks by the village/related agencies. Both of these programs/actions are highly relevant for implementing the policy of elderly care in their own homes.
4.1.2 Evaluation of the correlation between policy and scenarios
In addition to evaluating the correlation between policies and programs/actions, the correlation between policies and scenarios is also evaluated. In this study, two scenarios were previously explained: 1) The Care Model for Elderly Poor Living Alone/With a Partner; and 2) The Care Model for Non-Poor Elderly Living Alone/With a Partner. The correlation between policies and scenarios is presented in Table 3. In Table 3, several symbols/variables are provided.
The number reflects the ranking of policies based on the scenarios. The higher the number, the higher the rank, and vice versa. Therefore, if you want to create a ranking of policies, the largest number indicates the highest rank, and so on. Thus, the number already represents the rank of each policy. The value in the Number column also corresponds to the data in the Mean/average (Moy); the higher the average, the higher the ranking in the Number column, and vice versa. The value in Ec. Ty represents the standard deviation.
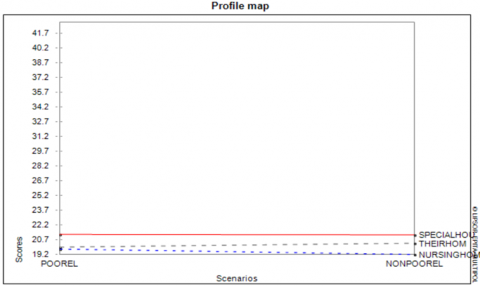
Based on the matrix in Table 3, it can be seen that the policy with the highest average value or the highest ranking is the Policy for Building Special Elderly Houses at the village level. The second rank is the Policy for Elderly Care at Their Homes, and the policy with the lowest rank is the Placement of the Elderly in Existing Nursing Homes. Table 3 can also be seen in Figure 5.
Table 3. Policy matrix for scenarios
|
|
POOREL |
NONPOOREL |
Moy. |
Ec. Ty |
Number |
|
SPECIALHOU |
21.3 |
21.2 |
21.3 |
0 |
3 |
|
NURSINGHOM |
19.8 |
19.2 |
19.5 |
0.3 |
1 |
|
THEIRHOM
|
20
|
20.4
|
20.2
|
0.2
|
2
|
Figure 5. Policy Profile Map for scenarios
Based on Figure 5, it can be seen in both scenarios—1) the Model for Elderly Care for Poor Elderly Living Alone/With a Partner, and 2) the Model for Elderly Care for Non-Poor Elderly Living Alone/With a Partner—that the policy with the highest score is the Policy for Building Special Elderly Houses at the village level. This suggests that, for both poor and non-poor families, elderly people should ideally have special houses built at the village level. However, in reality, the funds for building these special houses are limited. Therefore, when comparing the scores between the two groups, the score is higher for the poor families. Consequently, the policy of building special elderly houses at the village level is more suitable for Scenario 1, which focuses on elderly individuals from poor families.
The next policy is the Elderly Care at Their Homes policy, which ranks second in both scenarios. However, when looking at the scores for both scenarios, the score is higher in Scenario 2, for the non-poor elderly. Therefore, the Elderly Care at Their Homes policy is more appropriate for non-poor elderly individuals. However, in practice, there is a limitation in terms of the available workforce to conduct periodic home visits, not to mention the challenges posed by the long distances between the homes, requiring a significant amount of time to reach the elderly's homes.
Given that the highest score in both Scenario 1 and Scenario 2 is for the Policy for Building Special Elderly Houses at the village level, a possible compromise would be to combine both poor and non-poor elderly in one location. The final policy, Placement of the Elderly in Existing Nursing Homes, ranks third in both scenarios. However, looking at the score values for both scenarios, the policy of placing the elderly in existing nursing homes is more appropriate for the poor elderly, as seen in Scenario 1. Hurlock [36], cited in Wahidah [37], states that a good economic status allows someone to live comfortably and enjoy the good things in life in their old age. In contrast, a worsening economic status may force the elderly into a transition to a less desirable life, such as living in a nursing home. A decrease in income is often perceived as a move toward a smaller and less desirable life, such as living with married children or in a social institution like a nursing home. Considering all the score values in Table 3 and Figure 5, it can be concluded that the most suitable Elderly Care Model for both poor and non-poor elderly is the Policy for Building Special Elderly Houses at the village level.
4.1.3 The potential policy path that can be achieved is through the appropriate program for a specific policy and scenario
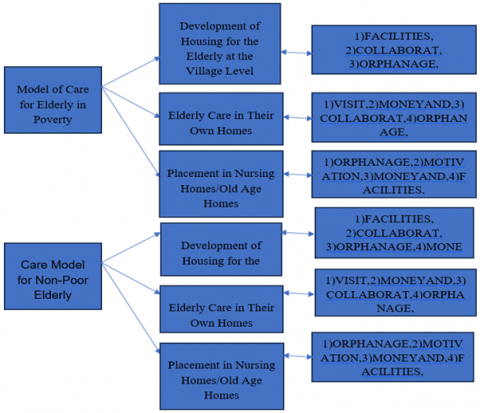
The final result of the multi-policy analysis as a whole can be presented in the form of a policy path with the appropriate program and scenario. The results of the previous multi-policy analysis include 2 scenarios, 3 policy alternatives, and 6 programs/actions. The results of the analysis are presented in Figure 6. Figure 6 shows the sequence of potential policies in each scenario, along with the sequence of corresponding programs in each policy. Each policy or different policy for both poor and non-poor elderly people has a different program sequence to achieve the designed policy. The multi-policy analysis also shows the ranking of policies from highest to lowest, with the same conditions for both poor and non-poor elderly. The first policy is the development of special housing for the elderly at the village level, the second ranking is elderly care at home, and the third ranking is placement in nursing homes. These elderly people are closely tied to their villages because they are still able to engage in various activities related to village customs and religion, making it difficult for them to leave their village to live in a nursing home. If care is provided at home, the social services or personnel are very limited in terms of visiting elderly people’s homes every day, considering the large coverage area and the relatively distant locations of the homes. Therefore, the most suitable policy, if funding permits, is the development of special housing for the elderly at the village level. Research in Beni-Suef Province, Egypt, on elderly people living in nursing homes also showed that 70 percent of the elderly had a low quality of life and 85 percent had limited knowledge about the changes associated with aging [38].
Figure 6. Potential policy paths and programs
4.2 The parties involved in determining the quality of life of the elderly
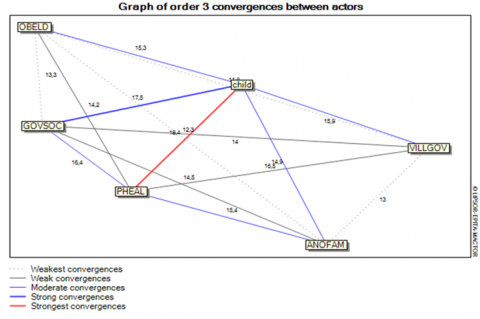
Research on the quality of life of the elderly is increasingly being conducted. Quality of life is defined as a comprehensive characteristic of physical, psychological, emotional, environmental, and social functions of patients, based on their subjective perceptions [39-41]. This also allows for the assessment of disease dynamics and the effectiveness of treatment. The elderly are a vulnerable group who are prone to experiencing various factors that affect their quality of life. The quality of life of the elderly is also related to their sensitivity to the taste of food they consume [42]. The elderly are a group that is highly dependent on their environment, similar to infants or children. Therefore, there must be parties that can contribute to improving the quality of life of the elderly. Based on the results of a FGD, several parties have been identified that play a role in determining the quality of life of the elderly in Karangasem Regency, including: 1) Children of the elderly (Child); 2) Other responsible family members (ANOFAM); 3) Government/Social Services (GOVSOC); 4) Village Government (VILLGOV); 5) Health Services (PHEAL); and Elderly Issue Advocates (OBELD). These parties have different roles in determining the quality of life of the elderly, and through Mactor Analysis, the relationships between these actors are shown in Figure 7.
Figure 7. Strength of the relationship between actors on the quality of elderly life
The data from the research shows that the role of various parties in determining the quality of life of the elderly is to maintain/preserve the health of the elderly as the top priority. Therefore, the health of the elderly becomes the most important factor if we want them to have a good quality of life. This is understandable because if the elderly are healthy, they will be able to do various things that contribute to their quality of life. Nothing can be done by the elderly if they are not healthy, whereas if they are healthy, they will be able to perform any activities. The second priority is to provide housing and meet other living needs of the elderly. For elderly individuals who previously did not have a home, this activity becomes very important to help maintain their health. The second activity is also vital in forming good physical health for the elderly. After ensuring physical health, the next role or activity in determining the quality of life is guiding the elderly to spiritual activities. Once the elderly are healthy and their physical needs, such as housing and daily needs, are met, the next step is fulfilling their spiritual needs. Providing supplementary food is another activity that can be done to maintain the health of the elderly so their quality of life remains intact. In certain conditions, such as during an epidemic, drought, or other exceptional circumstances, the important activity that can be performed is providing health assistance or incidental support for consumption. The last activity that must also be carried out is training the elderly to exercise in order to maintain their health. Essentially, all activities carried out for the elderly to contribute to their quality of life are aimed at preserving the health of the elderly. Quality of life is better for those who exercise regularly, but lower for those who suffer from obesity or diabetes [43].
Based on the sustainability analysis, which is the Mactor Analysis, the closeness of the relationships between the parties or actors in the effort to improve the quality of life of the elderly can be seen, as shown in Figure 6. In Figure 6, it can be seen that the relationship between the children and the Health Services is the strongest, meaning that children who are responsible for the health of their elderly parents will be closely related to the health services, as the elderly will need healthcare workers as they age. For the elderly, a deep understanding of their health aspects is needed to improve the system for a better quality of life and maximum independence [44]. Health education for the elderly is an important strategy used by health workers to encourage comprehensive care and support healthy and active aging [45]. The family function correlates positively with the quality of life of the elderly, so family involvement is necessary in the healthcare planning process to identify potential family stressors early and plan interventions to resolve emerging problems [6, 46]. Children (as the core family) and healthcare professionals (as the expert parties) share the same goal, which is to provide the best care and support for the elderly. Both parties do not work separately but support each other, communicate effectively, and share responsibilities well. The relationship between children and healthcare professionals is not just temporary but ongoing and consistent, creating a positive impact for the elderly. This relationship is shown to be very strong in this analysis (marked with a red line). The next relationship is between children and the Social Services Department, which has a strong connection, marked by a thick blue line. The community in the research area has the lowest welfare level compared to other regencies/cities in Bali Province, and therefore the elderly in this area are in similar, or even worse, economic conditions compared to other groups. The elderly will be very dependent on others, such as their children and other parties, making the role of the social services department very important in this regard. The strong convergence between children and the Social Services Department indicates synergistic efforts that can address challenges in areas with low welfare. The combination of emotional support from children and strategic assistance from Social Services creates a strong foundation to ensure that the elderly are respected, cared for, and receive a better quality of life, despite the challenging economic environment. The next relationship is between children and other family members, which has a moderate connection, not as strong as with the other parties, as other family members also have responsibilities to provide care for their closer family members. Similarly, elderly advocates and the village government have a moderate connection with children in efforts to improve the quality of life of the elderly.
Based on the results of the multi-policy analysis conducted for both poor and non-poor elderly, the policy is the Development of Special Elderly Houses at the village level. However, when considering the scores between the two scenarios, the policy is more appropriate for poor elderly individuals living alone or with a partner. The second policy is the Elderly Care at Home, but based on the scores between the two scenarios, this policy is more appropriate for non-poor elderly individuals. The third policy is the Placement of Elderly in Existing Nursing Homes/Retirement Homes, but considering the scores between the two scenarios, this policy is more suitable for poor elderly individuals living alone or with a partner.
Using the Mactor Analysis, it is evident that the convergence or strongest connection in efforts to improve the quality of life of the elderly is between the children and the health service, particularly health workers. The children and the social services also show a strong convergence or connection in efforts to improve the quality of life of the elderly. Other family members, elderly care advocates, and village governments have a moderate convergence or connection with the children in efforts to improve the elderly's quality of life.
In the analysis, it appears that the role of the village government is still relatively weak or low in improving the quality of life for the elderly at the village level. Therefore, the village government's role needs to be strengthened through various activities that can involve the elderly at the village level, such as health maintenance programs, elderly exercise programs, health checks, and other programs that support the elderly's quality of life. Additionally, in the policy of developing special elderly houses at the village level, the role of the village government is crucial to realizing elderly-friendly homes.
[1] Molina, N.P.F.M., Tavares, D.M.S., Haas, V.J., Rodrigues, L.R. (2020). Religiousity, spirituality and quality of life of elderly according to structural equation modeling. Texto & Contexto Enfermagem, 29: e20180468. https://doi.org/10.1590/1980-265X-TCE-2018-0468
[2] Anjos, C.A., Clemente, M., Dias, J.D.F.G., Burci, L.M., Leite, R.D.O., Miguel, M.D. (2022). Quality of life of elderly people living in different types of long-term care facilities. Brazilian Journal of Pharmaceutical Sciences, 58: e20117. https://doi.org/10.1590/S2175-97902022E20117
[3] Gruzieva, T.S., Diachuk, M.D., Inshakova, H.V., Soroka, I.M., Dufynets, V.A. (2021). Health of the elderly people as the basis for formation of medical and social needs. Wiadomości Lekarskie, 74(3 p.II): 658-664. https://doi.org/10.36740/WLEK202103217
[4] Song, M.K., Lee, H.J. (2021). Challenges of super aging: Socioeconomic and policy perspectives in South Korea. The Journals of Gerontology: Series B, 77(3): 589-596.
[5] Banio, A. (2020). The influence of Latin dance classes on the improvement of life quality of elderly people in Europe. Sustainability, 12(6): 2155. https://doi.org/10.3390/SU12062155
[6] Souza Júnior, E.V., Viana, E.R., Cruz, D.P., Silva, C.D.S., Rosa, R.S., Siqueira, L.R., Sawada, N.O. (2021). Relationship between family functionality and the quality of life of the elderly. Revista Brasileira de Enfermagem, 75(2): e20210106. https://doi.org/10.1590/0034-7167-2021-0106
[7] Barbosa, B.T., Santos, R.L.S.D., Meneses, A.B.C.D., Brindeiro-Neto, W., Bacurau, T.P., Rocha, A.I.S.D.S., Souza, L.I.S.D., Brasileiro-Santos, M.D.S. (2019). Self-related quality of life of elderly submitted to a 12-week aquatic training program. Journal of Human Sport and Exercise, 14(2): 281-291. https://doi.org/10.14198/JHSE.2019.142.03
[8] Kementerian PPN/Bappenas. (2020). Laporan Pelaksanaan Tujuan Pembangunan Berkelanjutan/SDGs Tahun 2020. Jakarta: Kementerian Perencanaan Pembangunan Nasional/Badan Perencanaan Pembangunan Nasional.
[9] Cahyani, R.D., Putri, S.W. (2025). The role of the government in the process of appointment of honorary and contract workers in Pasaman Regency. Priviet Social Sciences Journal, 5(10): 291-299. https://doi.org/10.55942/pssj.v5i10.876
[10] Issalillah, F., Aisyah, N. (2022). The elderly and the determinants of stress. Journal of Social Science Studies, 2(1): 9-12. https://doi.org/10.56348/JOS3.V2I1.19
[11] Joshi, M.R., Chalise, H.N. (2021). Elderly abuse and quality of life: A study of community living older people of Nepal. Journal of Medical Evidence, 2(2): 113-119. https://doi.org/10.4103/JME.JME_140_20
[12] Syamsuddin, S. (2022). The effect of information technology on the quality of financial reports in the regional financial management agency of Takalar Regency. Journal of Economics and Business Letters, 2(3): 8-11. https://doi.org/10.55942/jebl.v2i3.161
[13] Handayani, S. (2020). Bantuan sosial bagi lanjut usia di masa Pandemi. Journal of Social Development Studies, 1(2): 61-75. https://doi.org/10.22146/JSDS.657
[14] Ramadhan, M., Hidir, I. (2021). Dampak Program Keluarga Harapan (PKH) Terhadap Kesejahteraan Lansia di Indonesia. Jurnal Ilmiah Indonesia.
[15] Hidayat, B.W., Nuryadi, M.H., Rusnaini, R. (2019). Implementasi Program Keluarga Harapan terhadap pemenuhan hak sosial warga lansia miskin (Studi di Kecamatan Jebres Kota Surakarta). PKn Progresif: Jurnal Pemikiran dan Penelitian Kewarganegaraan, 14(1). https://doi.org/10.20961/PKNP.V14I1.34795
[16] Maifizar, A. (2016). Karakteristik dan fenomena kemiskinan keluarga miskin pedesaan di Aceh. Community Pengawas Dinamika Sosial, 2(3): 298-314. https://doi.org/10.35308/jcpds.v2i3.98
[17] Parwodiwiyono, S. (2022). Determinan Penduduk Lanjut Usia Miskindi Daerah Istimewa Yogyakarta. Jurnal Indonesia Sosial Sains, 3(3): 455-466. https://doi.org/10.59141/JISS.V3I03.510
[18] Kusumowardani, A., Puspitosari, A. (2014). Hubungan antara tingkat depresi lansia dengan interaksi sosial lansia di Desa Sobokerto, Kecamatan Ngemplak, Boyolali. Jurnal Terpadu Ilmu Kesehatan, 3(2): 184-188. https://id.scribd.com/document/948608180/Hubungan-Antara-Tingkat-Depresi-Lansia-D.
[19] Santoso, M.D.Y. (2019). Dukungan sosial meningkatkan kualitas hidup lansia: Review article. Jurnal Kesehatan Mesencephalon, 5(1): 33-41. https://doi.org/10.36053/mesencephalon.v5i1.104
[20] Nurhidayah, S., Agustini, R. (2012). Kebahagiaan lansia ditinjau dari dukungan sosial dan spiritualitas. Jurnal Soul, 5(2): 15-32. https://jurnal.unismabekasi.ac.id/index.php/soul/article/view/627.
[21] Thojampa, S., Daengthern, L., Kumpeera, K. (2020). The effects of an empowerment program to have a good quality of life and long life for elderly people in Phrae Province, Thailand. International Journal of Africa Nursing Sciences, 12: 100201. https://doi.org/10.1016/J.IJANS.2020.100201
[22] Alejandro, A.F., Rodrigo, V.V., Manuel, A., Miguel, M. (2021). Perception on the quality of life of elderly people during COVID-19 Pandemic in Chile. International Journal of Human Movement and Sports Sciences, 9(3): 473-479. https://doi.org/10.13189/SAJ.2021.090312
[23] Lee, C.J., Hsu, Y. (2021). Promoting the quality of life of elderly during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(13): 6813. https://doi.org/10.3390/IJERPH18136813
[24] Fauzi, A. (2019). Teknik Analisis Keberlanjutan. Jakarta: PT Gramedia Pustaka Utama.
[25] Suasih, N.N.R., Budhi, M.K.S. (2023). Mitigation policies for fashion SMEs affected by the COVID-19 Pandemic. General Management, 24(194): 274-284. https://doi.org/10.47750/QAS/24.194.31
[26] Wardono, B., Muhartono, R., Hikmayani, Y., Apriliani, T., Hikmah, H. (2019). Analisis prospektif peran aktor dalam strategi formulasi pembangunan perikanan di Kabupaten Natuna. Jurnal Sosial Ekonomi Kelautan dan Perikanan, 14(2): 179-195. https://doi.org/10.15578/JSEKP.V14I2.8241
[27] Ariyania, N., Fauzi, A., Umar, F. (2020). Model hubungan aktor pemangku kepentingan dalam pengembangan potensi pariwisata Kedung Ombo. Jurnal Ekonomi Dan Bisnis (JEB), 23(2): 357-378. https://doi.org/10.24914/JEB.V23I2.3420
[28] Effendi, N. (1998). Dasar-dasar keperawatan kesehatan masyarakat. Penerbit Buku Kedokteran EGC.
[29] Hart, J.T. (1971). The inverse care law. The Lancet, 297(7696): 405-412. https://doi.org/10.1016/S0140-6736(71)92410-X
[30] Radford, A.J. (1980). The inverse care law in Papua New Guinea. In Changing Disease Patterns and Human Behaviour.
[31] Zaidi, S.A. (1985). The urban bias in health facilities in Pakistan. Social Science & Medicine, 20(5): 473-482. https://doi.org/10.1016/0277-9536(85)90362-4
[32] Tamher, S., Noorkasiani. (2011). Kesehatan Usia Lanjut Dengan Pendekatan Asuhan Keperawatan. Jakarta: Salemba Medika.
[33] Darmojo, B., Martono, H. (2004). Buku Ajar Geriatri (Ilmu Kesehatan Usia Lanjut). Edisi ke-3. Jakarta: Balai Penerbit FKUI.
[34] Horner, B., Boldy, D.P. (2008). The benefit and burden of ageing-in-place in an aged care community. Australian Health Review, 32(2): 356-365. https://doi.org/10.1071/ah080356
[35] Adib, M. (2008). Penelitian lansia di perkotaan: Tinggal bersama keluarga lebih nyaman. http://madib.blog.unair.ac.id/files/2008/11/penelitian-Lansia-diperkotaan.pdf.
[36] Hurlock, E.B. (1997). Psikologi perkembangan: Suatu pendekatan sepanjang rentang kehidupan. Jakarta: Erlangga. https://library.stik-ptik.ac.id/detail?id=25662&lokasi=lokal.
[37] Wahidah, N. (2016). Pengaruh status ekonomi terhadap kesejahteraan lansia dan keputusan tempat tinggal. Jurnal Kesejahteraan Sosial, 17(1): 56-72.
[38] Mohamed, A.F., Mourad, G.M., Abd El-Fatah, W.O. (2020). Quality of life among elderly people at geriatric home. Niles Journal for Geriatric and Gerontology, 3(3): 271-283.
[39] Alexandrovna, I.O., Shodikulova, G.Z., Muxtorovna, E.M. (2023). Quality of life of elderly patients with osteoarthritis. Spectrum Journal of Innovation, Reforms and Development, 12: 145-155.
[40] Maung, T.M., Jain, T., Madhanagopal, J., Naidu, S.R.L.R., Phyu, H.P., Oo, W.M. (2022). Impact of aerobic and strengthening exercise on quality of life (QOL), mental health and physical performance of elderly people residing at old age homes. Sustainability, 14(17): 10881. https://doi.org/10.3390/SU141710881
[41] Wojcieszek, A., Kurowska, A., Majda, A., Kołodziej, K., Liszka, H., Gadek, A. (2023). Relationship between optimism, self-efficacy and quality of life: A cross-sectional study in elderly people with knee osteoarthritis. Geriatrics, 8(5): 101. https://doi.org/10.3390/GERIATRICS8050101
[42] Jeon, S., Kim, Y., Min, S., Song, M., Son, S., Lee, S. (2021). Taste sensitivity of elderly people is associated with quality of life and inadequate dietary intake. Nutrients, 13(5): 1693. https://doi.org/10.3390/NU13051693
[43] Song, J., Lee, E. (2021). Health-related quality of life of elderly women with fall experiences. International Journal of Environmental Research and Public Health, 18(15): 7804. https://doi.org/10.3390/IJERPH18157804
[44] González-Ojea, M.J., Domínguez-Lloria, S., Pino-Juste, M. (2022). Can music therapy improve the quality of life of institutionalized elderly people? Healthcare, 10(2): 310. https://doi.org/10.3390/HEALTHCARE10020310
[45] Seabra, C.A.M., Xavier, S.P.L., Sampaio, Y.P.C.C., Oliveira, M.F.D., Quirino, G.D.S., Machado, M.D.F.A.S. (2019). Health education as a strategy for the promotion of the health of the elderly: An integrative review. Revista Brasileira de Geriatria e Gerontologia, 22(4): e190022. https://doi.org/10.1590/1981-22562019022.190022
[46] Gallardo-Peralta, L.P., Sanchez-Moreno, E., Herrera, S. (2022). Aging and family relationships among aymara, mapuche and non-indigenous people: Exploring how social support, family functioning, and self-perceived health are related to quality of life. International Journal of Environmental Research and Public Health, 19(15): 9247. https://doi.org/10.3390/IJERPH19159247