Ryani Dhyan Parashakti*![]() | Achmad Sudiro
| Achmad Sudiro![]() | Sumiati
| Sumiati![]() | Mintarti
| Mintarti![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
This study investigates how institutional learning capacity contributes to the sustainable performance of public healthcare services through two workforce-related mechanisms—organizational commitment and organizational citizenship behavior (OCB)—and whether governance-related leadership practices condition these relationships. Using a cross-sectional survey of nurses from seven healthcare institutions operating under Indonesia’s National Health Insurance System (BPJS), 176 valid responses were analyzed using partial least squares structural equation modeling (PLS-SEM). The results indicate that institutional learning exerts a significant direct effect on workforce performance and indirectly enhances service sustainability through strengthened commitment and citizenship behavior. Organizational commitment and OCB both function as mediating mechanisms that translate learning into improved performance outcomes. Transformational leadership strengthens the effect of commitment on performance but weakens the contribution of OCB, suggesting that highly salient managerial interventions may reduce the voluntary and self-initiated nature of citizenship behaviors. The model explains a substantial proportion of variance in performance (R² = 0.845) and demonstrates predictive relevance. From a planning and policy perspective, the findings highlight the importance of investing in institutional learning systems, leadership development, and governance design to support sustainable public service delivery in healthcare. The study contributes to the sustainable development literature by demonstrating how organizational learning and human capital mechanisms interact to shape the long-term effectiveness and resilience of public healthcare systems.
institutional learning, public healthcare sustainability, workforce performance, organizational commitment, governance and leadership, sustainable development
The advent of the ASEAN Economic Community in 2015 increased pressures on healthcare systems to maintain service quality under rising demand and public expectations, placing sustained emphasis on the availability and stability of the nursing workforce. In Indonesia, accelerated health sector development has positioned hospitals as labor- and knowledge-intensive public service institutions that deliver not only medical and rehabilitative care but also education and research. This, in turn, requires leadership and organizational arrangements that can stabilize workforce commitment and support service continuity.
The COVID-19 pandemic further intensified these pressures. Nurses worked on the frontline with sustained exposure risks, mandatory direct contact, strict protective protocols, long working hours, and considerable social pressure, all of which increased stress and strained the work environment. In this context, nursing performance is not only an internal managerial concern but also an important accountability indicator and a visible sign of hospital service quality and public trust [1].
The literature has long emphasized the role of knowledge and learning in shaping the quality of work and organizational outcomes. Organizations that invest in learning are generally better able to adjust to environmental change and shifting demands. Knowledge is often described as a critical organizational resource that needs to be developed, maintained, and applied in a systematic way [2-4]. Organizational learning is therefore widely regarded as a central element of effective organizations and an important basis for renewal over time [5], while long-term performance depends on whether organizations are able to adapt as their external conditions evolve [6].
At the same time, empirical findings are not fully consistent. Although a positive relationship between learning and performance is frequently assumed, it is not always observed in field studies [7, 8]. Measurement approaches have improved and now allow learning cultures to be linked more clearly to organizational outcomes, but questions remain about how these constructs should be defined and operationalized [9].
Public service settings further complicate these dynamics. Bureaucratic structures, producer-consumer asymmetries, and administrative coercive power can constrain day-to-day work and make it harder to keep service orientation consistent, which is why explicit learning strategies become necessary in many public organizations [10]. At the same time, social health insurance reforms can expand access and push hospitals to improve quality. Indonesian Ministry of Health statistics record growth to 2,813 hospitals by end-2018 and highlight the legal entitlements to safe, quality, affordable care under the national social insurance framework [11]. As the system expands, the need for effective knowledge management becomes more visible in sectors marked by high fragmentation, rapid knowledge proliferation, and strong contextual dependence. Constraints on knowledge access, workforce aging, and knowledge attrition through retirement can undermine access, safety, and quality unless they are offset by continuing professional learning and deliberate staff development efforts [12].
Within hospitals, organizational learning has been linked to stronger employee commitment, clearer vision and goals, and closer alignment with service expectations [9, 13]. A learning culture is also associated with higher organizational commitment and job satisfaction, which can translate into better work outcomes [14]. Affective, continuance, and normative commitment provide different reasons for staying and investing effort, and these motives can be particularly salient in public or quasi-public settings where employment is shaped by budget constraints and formal performance evaluation [15]. At the unit level, nursing leadership influences structural empowerment and self-efficacy, which affects whether nurses can maintain professional practice behaviors under pressure [16]. Taken together, these arguments suggest that the effect of organizational learning on nurse performance may operate through organizational commitment and Organizational Citizenship Behavior (OCB), and that the strength of these relationships may depend on transformational leadership.
Empirical results, however, remain mixed. Some studies report significant effects of organizational learning on performance [17], while others report non-significant relationships, including cases where organizational commitment is modeled as a mediator [13]. These inconsistencies point to a gap in evidence from Indonesia’s public healthcare context, particularly among institutions serving National Health Insurance participants. Focusing on nurses in type D private hospitals in Jakarta, Indonesia, this study examines the effect of organizational learning on nurse performance, with organizational commitment and OCB as mediators and transformational leadership as a moderator.
The first foundation rests on Social Cognitive Theory, which evolved from Bandura’s Social Learning Theory and emphasizes learning as the result of reciprocal interactions among the individual, the environment, and behavior, with internal and external reinforcement and the role of past experience in shaping expectations and behavioral choices [18]. This theory explains how self-control and reinforcement direct behavior toward sustainable goals, while acknowledging limitations when environmental change does not automatically alter the individual, when the relative contributions of person, behavior, and context are not always clear, when biological and hormonal factors are overlooked, and when emotions and motivation are insufficiently accommodated, so that operationalization can become too broad to be fully tested within a single research design.
Building on this behavioral-cognitive foundation, the notion of organizational learning is positioned as a strategic capability that enables the creation, acquisition, integration, and dissemination of knowledge at the individual, team, organizational, and societal levels, with direct implications for innovation, customer value, and financial performance [9]. The terminological debate between organizational learning and the learning organization is clarified by distinguishing that the former emphasizes the process of learning, whereas the latter refers to an organizational form that facilitates it. This distinction also highlights that organizational learning requires intentional effort, a supportive culture, and integration within structural design to avoid the illusion of learning without real changes in routines [19]. In the Argyris and Schön framework, organizations act on “theories-in-use” that must be tested against outcomes; error detection and correction through reflective inquiry embed learning into shared images and organizational design, making the cycle of action, feedback, and revision the core of adaptation [20].
Empirically, organizational learning is associated with a range of constructive behavioral and attitudinal outcomes, such as commitment, self-efficacy, interpersonal trust, work engagement, satisfaction, and performance, and is also related to knowledge outcomes, such as innovation, knowledge creation, and knowledge transfer [21, 22]. Cross-context evidence shows positive correlations between organizational learning and actual and financial performance, although some findings indicate non-significant effects on innovation-based performance in particular settings, signaling the importance of sectoral contingencies and measurement design [23, 24]. This study adopts three dimensions of organizational learning from Sinkula et al. [25]: commitment to learning, shared vision, and open-mindedness, because they are relevant for capturing the intensity and direction of learning at the individual-team level in hospital services and nursing practice. Commitment to learning reflects the organization’s axiomatic value placed on learning activities and reflecting the causal consequences of actions; open-mindedness captures the capacity to relinquish obsolete mental models and facilitate unlearning; and a shared vision provides orientation that unifies energy, commitment, and learning priorities so that individuals understand expectations, outcome metrics, and the operative theories in use [26, 27].
Organizational commitment is a three-component construct that explains emotional attachment, cost-benefit considerations of membership continuity, and normative obligations to remain; together, these provide distinct psychological pathways that can motivate extra-role behavior and sustained effort toward organizational goals [28]. The literature states that commitment is closely linked to citizenship behavior, performance, and retention intentions; a strong, value-aligned organizational culture often strengthens commitment, while organizational support, justice, and leadership provide the context that fosters loyalty and affective investment [29-31]. Cross-country and cross-sector evidence confirms a positive association between commitment and performance, although several studies show heterogeneity, including differences in the impact of each component and conditions that weaken or nullify the direct influence of commitment on performance, thereby opening space for contextual mediators and moderators [15, 32].
OCB is defined as discretionary behavior beyond formal roles that is not directly recognized by reward systems, yet in aggregate enhances organizational effectiveness. Its forms include altruism, courtesy, civic virtue, conscientiousness, and sportsmanship, with conceptual variations proposed in the literature [33, 34]. In hospitals, the cross-professional team nature of work, coordination needs, time pressure, and service sensitivity make OCB crucial for clinical quality, service efficiency, and patient experience; limited OCB can reduce the quality of service delivery and damage the institutional image [35]. Evidence from other service sectors shows relationships between OCB, performance, and image, although the relationship with image can covary negatively when extra-role behavior is not supported by a fair climate and recognition. Therefore, HR policy design must balance the encouragement of OCB with perceptions of justice and workload [35, 36].
Transformational leadership provides an explanatory lens for how leaders influence increases members’ willingness to transcend self-interest, sustain intrinsic motivation, and align with a collective vision. Within the FRL model, transformational leadership consistently shows stronger associations with effectiveness and satisfaction than contingent rewards, whereas passive management-by-exception and laissez-faire tend to correlate negatively with outcomes [37-39]. To address discriminant validity critiques of the MLQ, this study follows the five-dimension interpretation by Rafferty and Griffin [40], which differentiates vision, inspirational communication, intellectual stimulation, supportive leadership, and personal recognition as more clearly defined and internally coherent behaviors. Vision articulates an ideal, values-based future that serves as a collective guide; inspirational communication mobilizes emotions and beliefs through positive messages; intellectual stimulation challenges assumptions, encourages new ways of thinking, and is linked to exploratory innovation; supportive leadership attends to follower needs and builds a collegial work environment; and personal recognition reinforces individual efforts and achievements so followers internalize the shared vision and goals [37, 41]. In nursing contexts, evidence shows that strong unit leadership broadens access to structural empowerment, enhances nurses’ self-efficacy, and promotes professional practice, while excessive workload and span of control can diminish leadership effectiveness [16, 42].
Nurse performance is understood as the effectiveness with which nurses complete patient care tasks and contribute to organizational goals and is theoretically distinguished into task performance and contextual performance. Nursing-specific measurements are required because generic scales are limited in capturing interpersonal support and clinical coordination [43, 44]. Structural factors such as education, experience, unit autonomy, time availability, and work strain have been identified as influencing coordination and communication. Social support from peers and supervisors is associated with higher performance and reduced stress, whereas the physical and social organizational climate also modulates satisfaction and absenteeism [45]. Performance-improvement models that emphasize clarity of expectations, feedback, environment and tools, motivation-incentives, and knowledge-skills show that training in clinical tools and recognition are intertwined with performance attainment [46].
A synthesis of prior studies reveals a pattern that is partly consistent and partly divergent from the current study. Several studies have linked organizational learning with commitment, satisfaction, and performance, with indications of partial mediation by commitment and satisfaction. Others have found a direct effect of learning on commitment and performance, but commitment does not directly affect performance, suggesting the need to consider more complex causal pathways [13, 47]. On the other hand, some findings show non-significant or even negative associations in particular subpopulations, such as younger cohorts, or the need for mediation by self-efficacy for learning to affect commitment, underscoring the importance of age heterogeneity, career norms, and psychological resources [14]. For OCB, the evidence points to contributions to performance and image, accompanied by caution about negative co-variation with image when extra effort is not accompanied by a climate that recognizes and fairly rewards discretionary work [35, 48, 49]. For commitment, meta-analyses generally show a positive correlation with performance, particularly for the affective and normative components, while continuance commitment may correlate negatively, confirming the need to map commitment profiles in public and healthcare settings [50]. Within this landscape, effective leadership emerges as an important facilitator of performance and competitive advantage, especially when organizations face innovation pressure and heightened competitive dynamics. Leadership plays a mediating and moderating role in the impact of learning practices, commitment, and OCB on performance outcomes [51].
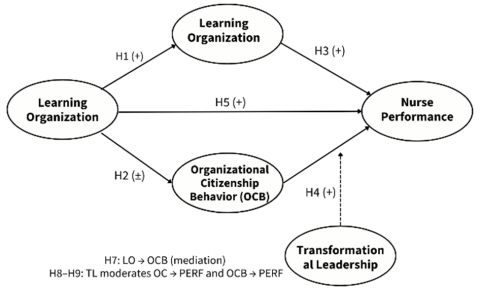
Figure 1. Conceptual framework
The conceptual framework of this study (Figure 1) positions organizational learning as the prime driver that affects nurse performance directly and indirectly through two key psychosocial mechanisms: organizational commitment and OCB. Commitment is projected as an affective-normative channel that enhances retention intention, persistence, and extra effort, whereas OCB functions as a discretionary behavioral channel that improves coordination, coworker support, discipline, participation, and resilience in nonideal situations. Both are influenced by learning experiences, unlearning, and a collective focus through a shared vision that unifies action orientation. In addition to these psychological and behavioral structures, transformational leadership is positioned as a contextual force that moderates the effectiveness of commitment and OCB in driving performance by strengthening structural empowerment, fostering self-efficacy, activating intrinsic motivation, and managing emotions and work meaning through vision and inspirational communication. Thus, the framework combines a direct path from learning to performance and two indirect paths through commitment and OCB, while testing whether leadership quality amplifies or reduces the strength of the commitment-performance and OCB-performance associations in the hospital ecosystem.
The operational constructs in this study were drawn from established instruments to preserve content and discriminant validity. Organizational learning is measured through three dimensions—commitment to learning, shared vision, and open-mindedness—as formulated by Sinkula et al. [25], because this measurement captures the axiomatic value of learning, the direction of learning, and the ability to release mental models that are no longer relevant to the organization. Organizational commitment is measured in the three components affective, normative, and continuance, following Meyer and Allen’s [28] framework, since each component reflects a different psychological motive for membership continuity and work investment. OCB is operationalized through the dimensions of altruism, courtesy, sportsmanship, civic virtue, and conscientiousness, in line with the tradition of Organ and Ryan [52], because these five dimensions represent discretionary contributions that typically appear in highly coordinated nursing settings. According to Greenslade and Jimmieson [43], nurse performance is differentiated into task performance and contextual performance, so that both the technical and extra-role aspects relevant to care quality can be captured. Transformational leadership follows the conceptual-empirical extension of Rafferty and Griffin [40] to the MLQ through five subdimensions—vision, inspirational communication, intellectual stimulation, supportive leadership, and personal recognition—which have theoretically and empirically shown coherence and improved discriminant validity over earlier dimensionalizations.
Based on this synthesis, the theoretical expectations tested include a positive relationship between organizational learning and nurse performance, both directly and through the mediation of commitment and OCB, with the effect of learning on commitment and OCB expected to be positive, as shown by studies linking learning culture with attachment and citizenship behavior. On the outcome side, nurse performance is expected to increase as commitment and OCB strengthen, with the heterogeneity of commitment components anticipated through the separate modeling of affective, normative, and continuance commitment. The above mediation relationships show that the quality of transformational leadership is assumed to reinforce the effects of commitment and OCB on performance, consistent with findings that unit leadership facilitates access to resources, heightens efficacy, and mobilizes collective energy toward more professional practice [16]. This framework is also adequate to accommodate earlier inconsistent findings, such as the nonsignificance of the commitment-performance path in certain contexts or differential generational effects, because the inclusion of leadership as a moderator enables testing the conditions under which these paths become strong or weak [13, 14].
By focusing on nurses in type-D private hospitals serving National Health Insurance participants in Jakarta, this model simultaneously examines how learning—channeled through shared values and vision as well as open-mindedness—interacts with the dynamics of commitment and citizenship behavior within a complex, bureaucratic public-service ecosystem. Emphasizing the role of transformational leadership links knowledge management policy with leadership development practices and recognition system design; thus, the resulting findings are expected to offer actionable guidance for interventions to improve care quality, retention, and nurse performance. Ultimately, the study’s conceptual contribution lies in integrating three learning-to-performance pathways that are mediated and moderated by key psychosocial variables while providing context-specific evidence from Indonesia, which remains underrepresented in hospital-based scholarship.
3.1 Population, sample, and data collection method
This study adopts a quantitative, positivist design with hypotheses derived from a theoretical review and empirical evidence. The unit of analysis was nurses at five hospitals in East Jakarta that actively serve National Health Insurance patients. The primary objective of this study is to explain the effect of organizational learning on nurse performance, with organizational commitment and OCB as mediators and leadership as a moderator. This approach is explanatory, aiming to test causal relationships among variables through hypothesis testing. The population comprised 1,994 nurses across five hospitals, which varied in size and service units. The sample consisted of 176 nurses who served National Health Insurance patients and had at least one year of tenure at the same hospital. Respondents were randomly selected to preserve representativeness and reduce selection bias.
Primary data were collected through structured questionnaires administered to nurses both offline and online, complemented by structured interviews and observations to strengthen the interpretation. Secondary data were obtained from internal hospital documents, literature, and scholarly journals. Measurement employed a five-point semantic differential scale treated as interval data, consistent with survey practice in business and management research that uses questionnaires and structured interviews as a unified set of data collection techniques presenting the same sequence of questions to each respondent [53]. The interpretation of response categories followed a mathematically derived Likert scale range to map respondents’ answer tendencies [54].
3.2 Variable instruments and tools of analysis
The instrument was developed from latent constructs operationalized using measurable indicators. Organizational learning, nurse performance, organizational commitment, OCB, and leadership were assessed using a five-point Likert scale. A pilot test involving 30 nurses from the five hospitals was conducted to assess preliminary validity and reliability of the questionnaire. Validity testing employed Confirmatory Factor Analysis within the SEM framework. Indicators were deemed valid when their factor loadings exceeded 0.60, whereas values below this threshold indicated that the indicators were inadequate to represent the construct [53]. CFA within SEM was chosen because it provides a stronger assessment of model validity and reliability than simpler techniques. Reliability was evaluated using composite reliability and Cronbach’s alpha internal consistency, with a Construct Reliability criterion of above 0.70 and a Variance Extracted of at least 0.50 to judge indicators as reliable and sufficiently explanatory of construct variance [53].
Hypothesis testing utilized Structural Equation Modeling (SEM) to estimate direct, indirect, and total relationships among latent variables, methodologically integrating factor analysis, regression, and path analysis within a single SEM framework [53, 55]. SEM was adopted because it is more accurate and robust for modeling interactions, nonlinearity, measurement errors, residual correlations, and covariances among latent variables. Theory-based model development began with a literature review and conceptual justification, followed by translation into a path diagram representing causal relationships with arrows, depicting latent variables as ellipses, and indicators as rectangles. The measurement model was evaluated using CFA, while the structural model tested the path coefficients among the constructs.
Model estimation and evaluation were conducted using LISREL, which separates measurement and structural models to depict the dimensions, variables, and interrelationships among latent variables simultaneously [56]. Model fit was assessed using absolute, incremental, and parsimony indices. RMSEA served as an informative indicator of model deviation from the population matrix, with a close fit at values less than or equal to 0.05 and a good fit in the range greater than or equal to 0.05 to 0.08. A GFI of at least 0.90 indicates accurate reproduction of the observed covariance matrix. NFI, AGFI, and IFI evaluated improvements in fit relative to a baseline model, with a 0.90 threshold as the criterion for a good fit and 0.80 to 0.90 interpreted as a marginal fit for NFI and AGFI. The PNFI and PGFI accounted for parsimony, where higher values reflected a more economical fit without sacrificing model clarity. Structural model evaluation was performed by assessing the significance and direction of path coefficients from exogenous to endogenous variables in line with theoretically specified hypotheses, including tests of the mediating effects of commitment and OCB, and the moderating role of leadership in their relationships with nurse performance. The analytical sequence began with the confirmation of instrument quality through validity and reliability testing, proceeded to model fit assessment, and concluded with the interpretation of structural parameters to address the research questions in the context of the National Health Insurance Service of East Jakarta, Indonesia.
4.1 Respondent characteristics
The unit of analysis comprised nurses from seven healthcare institutions in Jakarta that provide services to National Health Insurance patients. Table 1 summarizes the respondents’ characteristics.
Table 1. Respondent characteristics
|
Category |
n |
Percent (%) |
|
|
Gender |
Male |
56 |
31.8 |
|
Female |
120 |
68.2 |
|
|
Total |
176 |
100 |
|
|
Work length |
< 1 year |
11 |
6.3 |
|
1-5 year |
76 |
43.2 |
|
|
6-10 year |
38 |
21.6 |
|
|
> 10 year |
51 |
29 |
|
|
Total |
176 |
100 |
|
|
Education |
Diploma |
110 |
62.5 |
|
Undergraduate |
56 |
31.8 |
|
|
Master |
9 |
5.1 |
|
|
Doctoral |
1 |
0.6 |
|
|
Total |
176 |
100 |
|
|
Hospital |
RS. Yudika |
25 |
14.2 |
|
RS. Budi Asih |
27 |
15.3 |
|
|
RS. Pasar Rebo |
19 |
10.8 |
|
|
RS. Fatmawati |
24 |
13.6 |
|
|
PPNI (Persatuan Perawat Nasional Indonesia) Jakarta Selatan |
19 |
10.8 |
|
|
PPNI (Persatuan Perawat Nasional Indonesia) Jakarta Pusat |
30 |
17 |
|
|
RSIA Hermina |
32 |
18.2 |
|
|
Total |
176 |
100 |
|
Of the 176 usable questionnaires, the gender composition indicates a predominance of women, totaling 120 individuals (68.2%), while men accounted for 56 individuals (31.8%). Tenure is dominated by those with 1-5 years of experience, numbering 76 respondents (43.2%), followed by more than 10 years (51 respondents, 29.0%), 6-10 years (38 respondents, 21.6%), and less than 1 year (11 respondents, 6.3%). With respect to education, most hold a diploma (110 individuals or 62.5%), followed by a bachelor’s degree (56 individuals or 31.8%), master’s degree (nine individuals or 5.1%), and doctoral degree (one individual or 0.6%). All respondents worked in units serving the National Health Insurance. The distribution across institutions follows a proportional sampling design: RSIA Hermina 18.2 percent, PPNI Central Jakarta 17.0 percent, RS Budi Asih 15.3 percent, RS Yadika 14.2 percent, RSUP Fatmawati 13.6 percent, PPNI South Jakarta 10.8 percent, and RSUD Pasar Rebo 10.8 percent. This composition provides diversity in organizational contexts while preserving the representativeness of the study population.
4.2 Descriptive analysis of study variables
Response categorization was based on an index range of 1.00-5.00 with 0.80 intervals [57]. All five focal variables, organizational learning, organizational commitment, OCB, nurse performance, and transformational leadership, fell within the “good” category (Table 2).
Table 2. Descriptive analysis of research variables
|
No. |
Variable |
Total Score |
Maximum Score |
Average Score |
Category |
|
1 |
Organizational Learning |
4068 |
5280 |
3.852 |
Good |
|
2 |
Organizational Commitment |
4267 |
5280 |
4.041 |
Good |
|
3 |
Organizational Citizenship Behavior |
6958 |
8800 |
3.953 |
Good |
|
4 |
Nurse Performance |
2732 |
3520 |
3.881 |
Good |
|
5 |
Transformational Leadership Style |
6796 |
8800 |
3.861 |
Good |
Organizational Commitment was the highest (M = 4.041, SD = 0.835), indicating a strong attachment and willingness to contribute. OCB follows closely (M = 3.954, SD = 0.864), suggesting frequent discretionary helping behavior. Nurse Performance (M = 3.881, SD = 0.839), Transformational Leadership (M = 3.861, SD = 0.914), and Organizational Learning (M = 3.852, SD = 0.884) were also rated favorably.
Within organizational learning, the highest score pertained to the hospital’s openness to nurses’ criticism and suggestions, indicating a relatively active feedback culture, whereas the weakest area was the socialization of the vision and mission, highlighting a clear avenue for improvement. For organizational commitment, the strongest indicator was willingness to remain despite remuneration delays, whereas pride in working at the hospital was comparatively lower. In OCB, understanding duties and responsibilities recorded the highest score, while perceptions of collaborating to solve problems together were relatively weaker. For nurse performance, the readiness to devote additional working time emerged as the strongest indicator. In transformational leadership, forward-looking vision scored the highest, whereas leadership communication was rated comparatively lower. These patterns are instructive for sharpening recommendations to strengthen learning processes, clarify the vision and mission, reinforce team collaboration, and improve leadership communication.
4.3 SEM-PLS analysis
4.3.1 Measurement model (outer model)
Convergent validity was evaluated using factor loadings and average variance extracted (AVE), while reliability was assessed via Composite Reliability and Cronbach’s alpha [55]. All indicators across the five core constructs exhibited loadings above 0.70, average variance extracted (AVE) values exceeding 0.50, and composite reliability (CR) and alpha values above 0.70. Accordingly, all constructs were valid and reliable, consistent with best practices in survey research employing latent constructs. These results reinforce the soundness of the instrument, which had been pilot-tested beforehand.
The Fornell-Larcker criterion shows that the square root of the AVE for each construct is greater than its correlation with other constructs, indicating adequate construct separation (Table 3).
Given the recognized limitations of the Fornell-Larcker approach in detecting discriminant validity problems in some cases, HTMT was also applied. Bootstrapping with 5,000 samples produced confidence intervals that did not exceed 1.00, indicating no discriminant validity issues [58]. Cross-loadings further confirmed that each indicator loaded higher on its intended construct than on any alternative.
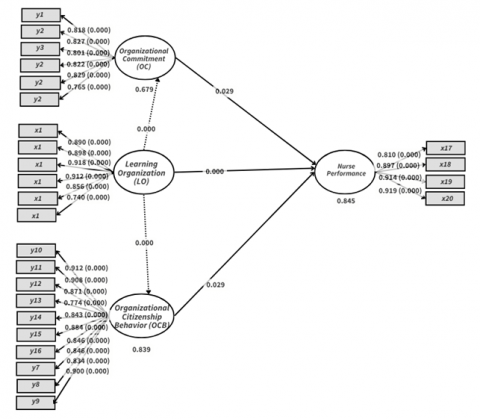
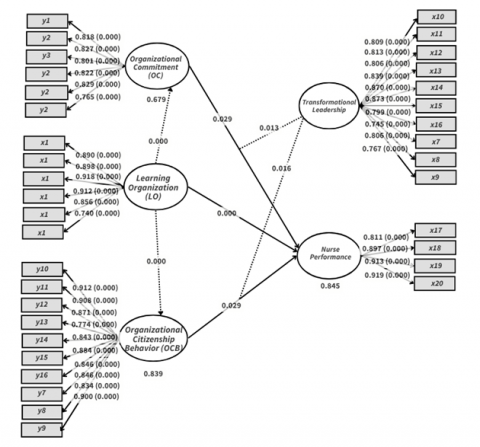
Two specifications were estimated, with and without the interaction term for transformational leadership. Without moderation (Figure 2), the path coefficients were 0.463 from organizational learning to nurse performance, 0.162 from organizational commitment to performance, 0.326 from OCB to performance, 0.824 from learning to commitment and 0.916 from learning to OCB. With moderation (Figure 3), the commitment-performance path increased to 0.185, whereas the OCB-performance path decreased to 0.241. The interaction of transformational leadership with commitment yielded a coefficient of 0.173, strengthening the effect on performance, while its interaction with OCB was −0.171, weakening the effect of OCB on performance. The R² for performance increased from 0.833 to 0.845 after including moderation, indicating the additional explanatory role of transformational leadership.
The model explains a large share of the variance in the endogenous constructs. Without the moderation term, the R² for Nurse Performance was 0.833; with moderation, it rose to 0.845. Following Hair et al. [59], R² values of 0.25-0.49 are weak, 0.50-0.74 moderate, and ≥ 0.75 strong, placing both specifications firmly in the “strong” range. R² represents the proportion of variance in an endogenous construct accounted for by its predictors and ranges from zero to one. Higher values indicate better explanatory power, although a well-known caveat is that R² tends to increase whenever predictors are added, even if they are not statistically meaningful.
Table 3. Validity test result
|
Transformational Leadership |
Nurse Performance |
Organizational Commitment |
Organizational Citizenship Behavior |
Organizational Learning |
|
|
Transformational Leadership |
0.914 |
||||
|
Nurse Performance |
0.862 |
0.886 |
|||
|
Organizational Commitment |
0.874 |
0.813 |
0.91 |
||
|
Organizational Citizenship Behavior |
0.888 |
0.883 |
0.828 |
0.916 |
|
|
Organizational Learning |
0.907 |
0.794 |
0.824 |
0.844 |
0.971 |
Figure 2. Baseline PLS-SEM structural model without moderation
Figure 3. Moderated PLS-SEM
Detailing the constructs: in the model without moderation, the R² (adjusted) values are 0.833 (0.830) for Nurse Performance, 0.679 (0.677) for Organizational Commitment, and 0.839 (0.838) for OCB. With transformational leadership included as an interaction, the R² for Nurse Performance increased to 0.845 (adjusted 0.840), while Commitment (0.679) and OCB (0.839) remained unchanged. Substantively, organizational learning, organizational commitment, and OCB explained 83.3% of the variance in nurse performance in the baseline model; adding the moderation term increased this to 84.5%, a 1.2 percentage-point gain. The remaining 15.5-16.7% likely reflects unmodeled factors such as work motivation, compensation, and broader organizational culture.
The predictive relevance (Q²) assesses how well the model reproduces the observed values. According to Hair et al. [59], Q² > 0 indicates predictive relevance. All endogenous constructs met this criterion across both specifications. For Nurse Performance, Q² predict was 0.798 (RMSE = 0.457; MAE = 0.340) without moderation and 0.802 (RMSE = 0.452; MAE = 0.333) with moderation. Organizational Commitment records Q² predict = 0.673 (RMSE = 0.584; MAE = 0.440) in both models, and OCB records 0.836 (RMSE = 0.411; MAE = 0.307) in both. These values indicate a meaningful out-of-sample predictive capability.
Model fit was evaluated using the standardized root mean square residual (SRMR), which is the standardized average discrepancy between observed and model-implied correlations, and the normed fit index (NFI), which is a comparative fit measure. The recommended thresholds are SRMR < 0.10 (preferably < 0.08), and NFI > 0.90 [59]. In the model without moderation, the SRMR was 0.064 (saturated) and 0.067 (estimated), indicating a good fit, whereas the NFI values of 0.872 and 0.870 fell slightly short of the 0.90 benchmark (marginal fit). In the moderated model, the SRMR remained acceptable at 0.069 (saturated) and 0.076 (estimated), and the NFI improved substantially to 0.965 and 0.958, exceeding the threshold. Additional indices (d_ULS, d_G, Chi-square) are reported for completeness, although no firm cutoffs apply. Overall, the moderated specification satisfies both the SRMR and NFI criteria and is therefore suitable for substantive inference.
4.3.2 Results
This study incorporates transformational leadership as a moderating construct in the structural model to test whether it strengthens or weakens the direct effects of organizational commitment and OCB on the performance of nurses. The results of the path analyses address these questions and adjudicate the study hypotheses (Table 4).
The findings indicate dual mediation: both organizational commitment and OCB transmit the positive effect of organizational learning on nurse performance. Beyond these indirect pathways, transformational leadership operates as a contingent enhancer of the commitment-performance link, yet it weakens the OCB-performance association. Specifically, the interaction term between transformational leadership and organizational commitment is positive (β = 0.173), implying that leaders who articulate vision, stimulate intellect, and provide individualized consideration convert employees’ commitment into higher performance more effectively than others. In contrast, the interaction between transformational leadership and OCB was negative (β = −0.171). Substantively, when leadership intervention becomes overly directive or salient, the discretionary and voluntary essence of OCB may diminish—employees perceive less autonomy or feel more monitored—thereby weakening OCB’s contribution to the performance. In light of this countervailing pattern, the final model recommends dropping the moderation path from transformational leadership to the OCB-performance relationship, because there is no theoretical or empirical support for a strengthening effect.
Table 4. Summary of path analysis results
| No. | Hypothesis | Path Coefficient (Without Interaction) | Path Coefficient (With Interaction) | t-Statistic (Without Interaction) | t-Statistic (With Interaction) | P-Value | Decision |
| 1 | Effect of Organizational Learning on Nurse Performance | 0.463 | 0.394 | 4.991 | 3.783 | 0 | Accepted |
| 2 | Effect of Organizational Learning on Organizational Commitment | 0.824 | 0.824 | 27.49 | 27.491 | 0 | Accepted |
| 3 | Effect of Organizational Learning on Organizational Citizenship Behavior (OCB) | 0.916 | 0.916 | 63.077 | 63.076 | 0 | Accepted |
| 4 | Effect of Organizational Commitment on Nurse Performance | 0.162 | 0.185 | 2.228 | 2.185 | 0.026 | Accepted |
| 5 | Effect of OCB on Nurse Performance | 0.326 | 0.241 | 2.802 | 2.19 | 0.005 | Accepted |
| 6 | Mediating Role of Organizational Commitment in the Relationship between Organizational Learning and Nurse Performance | 0.133 | 0.153 | 2.225 | 2.172 | 0.026 | Accepted |
| 7 | Mediating Role of OCB in the Relationship between Organizational Learning and Nurse Performance | 0.298 | 0.221 | 2.801 | 2.185 | 0.005 | Accepted |
| 8 | Moderating Role of Transformational Leadership in the Relationship between Organizational Commitment and Nurse Performance | 0.173 | — | 2.481 | — | 0.013 | Accepted |
| 9 | Moderating Role of Transformational Leadership in the Relationship between OCB and Nurse Performance | −0.171 | — | 2.416 | — | 0.016 | Accepted |
Path analysis was used to partition the direct and indirect effects among organizational learning, organizational commitment, OCB, and nurse performance. Without the interaction terms, the direct effect of organizational learning on performance is β = 0.463 (t = 4.991, p < 0.001), which remains significant in the moderated model, although attenuated (β = 0.394, t = 3.783, p < 0.001). Organizational learning strongly predicted both mediators: commitment (β = 0.824; t ≈ 27.49; p < 0.001) and OCB (β = 0.916; t ≈ 63.08; p < 0.001) in models with and without moderation.
As shown in Figure 4, organizational commitment exhibited a positive direct association with nurse performance (β = 0.162; t = 2.228; p = 0.026), which became slightly stronger when leadership interaction was included (β = 0.185; t = 2.185; p = 0.026). OCB also has a positive direct effect on performance in the baseline model (β = 0.326; t = 2.802; p = 0.005), which decreases after including the interaction (β = 0.241; t = 2.190; p = 0.005), consistent with the negative moderation noted above.
Mediation tests confirmed that commitment and OCB carry significant portions of the learning-performance linkage (Figure 5). The indirect effect via commitment was β = 0.133 (t = 2.225; p = 0.026) without moderation and β = 0.153 (t = 2.172; p = 0.026) with moderation. The indirect effect via OCB is β = 0.298 (t = 2.801; p = 0.005) without moderation and β = 0.221 (t = 2.185; p = 0.005) with moderation. These results show that organizational learning enhances performance directly and operates through heightened commitment and citizenship behavior.
This study has two implications. First, transformational leadership amplifies the performance returns to organizational commitment. Hospitals and health systems that invest in leadership development—coaching, visioning, recognition, and individualized support—are likely to see greater performance dividends from committed nurses. Second, the same leadership behaviors can inadvertently suppress the naturally discretionary character of OCB if they are enacted too intensively. OCB thrive in climates of autonomy, trust, and psychological safety; excessive oversight risks converting voluntary helping into perceived obligation, weakening its performance utility. Therefore, managers should calibrate transformational behaviors: inspire and scaffold but preserve space for initiatives so that citizenship behaviors remain authentic and impactful.
Figure 4. PLS-SEM structural model without moderation
Figure 5. PLS-SEM structural model with moderation
Statistically, all primary hypotheses are supported at the 5% level (one-tailed), with t-statistics exceeding the critical value (≈ 1.65) and p-values below 0.05. The moderated model explains a substantial share of variance in nurse performance (R² = 0.845) and maintains predictive relevance (Q² > 0, for all endogenous constructs). Taken together, the evidence positions organizational learning as a foundational driver of performance—operating directly and through commitment and OCB—while highlighting transformational leadership as a conditional catalyst for commitment-driven performance and a potential brake on the performance returns of OCB when enacted too strongly. Therefore, balancing inspiration with autonomy is essential for sustaining high performance in nursing contexts.
4.3.3 Discussion
The first hypothesis was supported. Higher organizational learning is associated with improved nursing performance. Theoretically, organizations that can create, store, access, and disseminate knowledge enhance both individual and collective capacities. Learning is accelerated by collaborative HRM practices and knowledge-sharing infrastructure, which, in turn, shape work outcomes such as satisfaction and performance [21]. Cross-context evidence broadly supports this positive link [13, 47, 60], although context-specific exceptions exist, such as Calisir et al. [61] in Turkey for innovation-based performance. In this study, the mean score for organizational learning fell in the “good” category, the indicators were valid, and the structural correlations were significant, reinforcing the argument that systematic investment in learning processes elevates nurse performance, especially for the 1-5-year experience group that dominates the sample and requires practical competence enrichment.
The second hypothesis was supported. Increases in organizational learning raise nurses’ commitment. Prior studies have shown that organizational learning exerts a direct effect on commitment and performance, though not necessarily the reverse [13, 47, 62]. Generational heterogeneity may moderate this link, as D'Amato and Herzfeldt [14] reported a negative association among post-1960 cohorts. Within a work behavior framework, belief in organizational values and goals, willingness to exert effort, and desire to remain with the organization function as psychological mechanisms tying learning to commitment. The mean commitment level in this study was “good,” suggesting a relatively supportive environment. Strengthening formal and informal learning channels and career mentoring is likely to further consolidate attachment, although several studies emphasize the need for personal mediators, such as self-efficacy, to optimize the effect [63].
The third hypothesis is thus supported. The structures and values of learning were positively correlated with OCB, consistent with Somech and Drach-Zahavy [64] and Islam et al. [65]. In hospital settings, collective learning nurtures a culture of mutual assistance, initiative, and willingness to go beyond formal role requirements. In this study, the mean OCB score fell in the “good” category, and its indicators were valid, suggesting that policies encouraging team reflection, case discussions, and learning communities can further strengthen OCB. Given that the respondent pool is dominated by women and diploma graduates, practice-based collaborative approaches and clinical coaching are likely to be more effective in the future.
The fourth hypothesis is thus supported. Commitment is positively associated with performance, aligning with literature that positions commitment as a determinant of engagement and work output [28, 66]. Meta-analytic evidence points to a consistent positive relationship, particularly for affective and normative dimensions, whereas continuance commitment sometimes negatively correlates with performance [50]. Contextual differences can yield non-significant results in some studies [67, 68]. In the National Health Insurance context in Jakarta, strong commitment driven by a sense of public service and organizational support appears to be the key explanation for improved nurse performance.
The fifth hypothesis is thus supported. OCB enhances nurse performance, consistent with the findings in hospitals and various service organizations [35, 49]. This mechanism operates through improved coordination, team efficiency, and service quality. Kolade et al. [35], however, note a negative covariance between OCB and corporate image under certain conditions, given the possibility of role fatigue when OCB is not well managed. Therefore, organizations need to balance recognition and rewards to foster healthy and sustainable OCB.
The sixth hypothesis was supported. Commitment mediates the effect of organizational learning on performance. Effective learning strengthens individual identification with and attachment to the organization, thereby encouraging greater discretionary effort, persistence, and quality orientation, which, in turn, elevates work outcomes [31, 69]. Given that the nurses had 1-5 years of experience, reinforcing career pathways, recognizing competencies, and implementing performance-based feedback were pivotal for amplifying this mediating effect.
The seventh hypothesis was supported. OCB have emerged as psychosocial mechanisms that bridge learning and performance. Cross-context evidence shows that OCB mediates the impact of personal learning on organizational performance, including in Chinese family firms [70], and in a large-scale study in Korea [71]. In hospital settings, learning that emphasizes team reflection and continuous improvement stimulates voluntary behaviors relevant to patient safety and service quality, which ultimately manifests in individual and unit performance.
The eighth hypothesis is thus supported. The interaction of transformational leadership strengthens the influence of commitment on performance. Leaders who articulate a compelling vision, motivate, provide intellectual stimulation, and offer individualized consideration can translate nurses’ commitment into high-performance behaviors. The literature underscores the centrality of leadership in hospital organizations in enhancing staff capability and performance [16]. Among early- to mid-career nurses, leadership that delivers coaching, reinforces the public value of care work, and grants professional autonomy is likely to magnify the effect of commitment on performance.
The ninth hypothesis was supported in the negative direction. The interaction between transformational leadership and OCB weakens the influence of OCB on performance. This finding opens a new dialectic: when leadership intervention becomes overly intensive, discretionary behaviors that should arise spontaneously may diminish because employees feel monitored or instructed, eroding the voluntary essence of the OCB. From an organizational design perspective, OCB flourishes within a psychological space that affords autonomy, trust, and safety to act beyond the formal job description. Therefore, leadership strategies should balance inspiration and direction with room for initiative so that OCB remains authentic and yields a maximal impact on performance.
Organizational learning plays a central role in shaping workforce performance, strengthening organizational commitment, and fostering OCB in healthcare settings. The findings reinforce the view that institutions that invest in continuous learning are better able to support employee capability and, in turn, maintain service quality in demanding clinical environments. The mediating role of organizational commitment highlights that learning does not operate as a simple or direct lever of performance, but rather works through layered psychological and behavioral mechanisms.
Building on these insights, this study proposes the Nursing Organizational Learning Enhancement (NOLE) Model as a way of explaining how learning processes within healthcare organizations shape commitment, citizenship behavior, and performance. In health systems where service quality, safety, and continuity are ongoing concerns, these mechanisms have practical implications for how institutions sustain their human resources over time. Learning structures do not only develop skills; they also influence whether professionals remain engaged, willing to cooperate, and prepared to respond to increasing demands and uncertainty.
By clarifying the pathways linking learning, commitment, citizenship behavior, and performance, the NOLE Model offers a framework for understanding how internal organizational practices connect to broader service outcomes. The study therefore contributes to discussions on healthcare workforce capacity and institutional capability, and provides a basis for decision-makers and practitioners to think about how learning and development policies can support long-term service effectiveness. In this sense, organizational learning emerges not only as an empirical driver of performance, but also as a foundation for sustaining the quality and reliability of public healthcare services.
[1] Kuntjoro, T. (2005). Performance management development for nurses and midwives as a national strategy for improving quality of clinical care. Jurnal Manajemen Pelayanan Kesehatan, 8(3): 149-154. https://d1wqtxts1xzle7.cloudfront.net/35432565/2650mmmm-libre.pdf?1415215505.
[2] Alam, A., Hartitah, F.A., Nordin, N. (2025). The influence of Islamic leadership on the creativity of employees of sharia microfinance institutions: The role of knowledge sharing and organizational innovation. Journal of Research Innovation and Technologies (JoRIT), 4(3): 283-296. https://doi.org/10.56578/jorit040304
[3] Chatterjee, S., Mousumi, S. (2023). Knowledge management: A tool and technology for organizational success. Journal of Research, Innovation and Technologies (JoRIT), 2(16): 7. https://doi.org/10.57017/jorit.v2.1(3).01
[4] Kocoglu, I., Imamoglu, S.Z., Ince, H. (2011). The relationship between organizational learning and firm performance: The mediating roles of innovation and TQM. Journal of Global Strategic Management, 1(5): 72. https://doi.org/10.20460/jgsm.2011515814
[5] Watkins, K.E., Kim, K. (2017). Current status and promising directions for research on the learning organization. Human Resource Development Quarterly, 29(1): 15-29. https://doi.org/10.1002/hrdq.21293
[6] Reese, S. (2020). Taking the learning organization mainstream and beyond the organizational level. The Learning Organization, 27(1): 6-16. https://doi.org/10.1108/tlo-09-2019-0136
[7] Sidani, Y., Reese, S. (2018). A journey of collaborative learning organization research. The Learning Organization, 25(3): 199-209. https://doi.org/10.1108/tlo-01-2018-0015
[8] Spicer, D.P., Sadler-Smith, E. (2006). Organizational learning in smaller manufacturing firms. International Small Business Journal: Researching Entrepreneurship, 24(2): 133-158. https://doi.org/10.1177/0266242606061836
[9] Marsick, V.J., Watkins, K.E. (2003). Demonstrating the value of an organization's learning culture: The dimensions of the learning organization questionnaire. Advances in Developing Human Resources, 5(2): 132-151. https://doi.org/10.1177/1523422303005002002
[10] Durrah, O.M., Allil, K.K., Alkhalaf, T. (2018). The intellectual capital and the learning organization. International Journal of Public Leadership, 14(2): 109-118. https://doi.org/10.1108/ijpl-08-2017-0031
[11] Putri, N.E. (2014). Efektivitas penerapan jaminan kesehatan nasional melalui BPJS dalam pelayanan kesehatan masyarakat miskin di kota Padang. Tingkap, 10(2): 175-189.
[12] Littlejohn, L., Campbell, J., Collins McNeil, J. (2012). Comparative analysis of nursing shortage. International Journal of Nursing, 1(1): 23-27.
[13] Khunsoonthornkit, A., Panjakajornsak, V. (2018). Structural equation model to assess the impact of learning organization and commitment on the performance of research organizations. Kasetsart Journal of Social Sciences, 39(3): 457-462. https://doi.org/10.1016/j.kjss.2018.07.003
[14] D'Amato, A., Herzfeldt, R. (2008). Learning orientation, organizational commitment and talent retention across generations. Journal of Managerial Psychology, 23(8): 929-953. https://doi.org/10.1108/02683940810904402
[15] Meyer, M. (2002). Managing Human Resource Development: An Outcomes-Based Approach. LexisNexis Butterworths.
[16] Manojlovich, M. (2005). The effect of nursing leadership on hospital nurses' professional practice behaviors. JONA: The Journal of Nursing Administration, 35(7): 366-374. https://doi.org/10.1097/00005110-200507000-00009
[17] Antunes, H.D.J.G., Pinheiro, P.G. (2020). Linking knowledge management, organizational learning and memory. Journal of Innovation & Knowledge, 5(2): 140-149. https://doi.org/10.1016/j.jik.2019.04.002
[18] Bandura, A. (1986). Social Foundations of Thought and Action: A Social Cognitive Theory. Prentice-Hall, Inc.
[19] Ortenblad, A. (2001). On differences between organizational learning and learning organization. The Learning Organization, 8(3): 125-133. https://doi.org/10.1108/09696470110391211
[20] Argyris, C., Schön, D.A. (1997). Organizational learning: A theory of action perspective. Reis, (77/78): 345. https://doi.org/10.2307/40183951
[21] Dirani, K.M. (2009). Measuring the learning organization culture, organizational commitment and job satisfaction in the Lebanese banking sector. Human Resource Development International, 12(2): 189-208. https://doi.org/10.1080/13678860902764118
[22] Hernandez, M., Watkins, K. (2003). Translation, validation and adaptation of the Spanish version of the modified dimensions of the learning organization questionnaire. Human Resource Development International, 6(2): 187-196. https://doi.org/10.1080/13678860110087923
[23] Awasthy, R., Gupta, R.K. (2012). Dimensions of the learning organization in an Indian context. International Journal of Emerging Markets, 7(3): 222-244. https://doi.org/10.1108/17468801211236956
[24] Ellinger, A.D., Ellinger, A.E., Yang, B., Howton, S.W. (2002). The relationship between the learning organization concept and firms' financial performance: An empirical assessment. Human Resource Development Quarterly, 13(1): 5-22. https://doi.org/10.1002/hrdq.1010
[25] Sinkula, J.M., Baker, W.E., Noordewier, T. (1997). A framework for market-based organizational learning: Linking values, knowledge, and behavior. Journal of the Academy of Marketing Science, 25(4): 305-318. https://doi.org/10.1177/0092070397254003
[26] Nystrom, P.C., Starbuck, W.H. (1984). To avoid organizational crises, unlearn. Organizational Dynamics, 12(4): 53-65. https://doi.org/10.1016/0090-2616(84)90011-1
[27] Senge, P.M. (1990). The Fifth Discipline: The Art and Practice of the Learning Organization. Doubleday/Currency.
[28] Meyer, J.P., Allen, N.J. (1991). A three-component conceptualization of organizational commitment. Human Resource Management Review, 1(1): 61-89. https://doi.org/10.1016/1053-4822(91)90011-z
[29] Armstrong, G., Adam, S., Denize, S., Kotler, P. (2014). Principles of Marketing. Pearson Australia.
[30] Luthans, F., Luthans, B.C., Luthans, K.W. (2021). Organizational Behavior: An Evidence-Based Approach (14th ed.). IAP.
[31] Carlos Pinho, J., Paula Rodrigues, A., Dibb, S. (2014). The role of corporate culture, market orientation and organisational commitment in organisational performance. Journal of Management Development, 33(4): 374-398. https://doi.org/10.1108/jmd-03-2013-0036
[32] Tsai, A. (2014). An empirical model of four processes for sharing organisational knowledge. Online Information Review, 38(2): 305-320. https://doi.org/10.1108/oir-03-2013-0059
[33] Podsakoff, P.M., MacKenzie, S.B., Paine, J.B., Bachrach, D.G. (2000). Organizational citizenship behaviors: A critical review of the theoretical and empirical literature and suggestions for future research. Journal of Management, 26(3): 513-563. https://doi.org/10.1177/014920630002600307
[34] Turnipseed, D.L., Rassuli, A. (2005). Performance perceptions of organizational citizenship behaviours at work: A bi-level study among managers and employees. British Journal of Management, 16(3): 231-244. https://doi.org/10.1111/j.1467-8551.2005.00456.x
[35] Kolade, O., Ogunnaike, O., A., O. (2014). Organizational citizenship behaviour, hospital corporate image and performance. SSRN Electronic Journal. https://doi.org/10.2139/ssrn.3047861
[36] Yen, H.R., Niehoff, B.P. (2004). Organizational citizenship behaviors and organizational effectiveness: Examining relationships in Taiwanese banks. Journal of Applied Social Psychology, 34(8): 1617-1637. https://doi.org/10.1111/j.1559-1816.2004.tb02790.x
[37] Bass, B.M. (1985). Leadership: Good, better, best. Organizational Dynamics, 13(3): 26-40. https://doi.org/10.1016/0090-2616(85)90028-2
[38] Bass, B.M., Avolio, B.J. (1994). Improving Organizational Effectiveness Through Transformational Leadership. SAGE.
[39] Bass, B.M., Riggio, R.E. (2006). Transformational Leadership. Psychology Press. https://doi.org/10.4324/9781410617095
[40] Rafferty, A.E., Griffin, M.A. (2004). Dimensions of transformational leadership: Conceptual and empirical extensions. The Leadership Quarterly, 15(3): 329-354. https://doi.org/10.1016/j.leaqua.2004.02.009
[41] Goodwin, V.L., Wofford, J.C., Whittington, J.L. (2001). A theoretical and empirical extension to the transformational leadership construct. Journal of Organizational Behavior, 22(7): 759-774. https://doi.org/10.1002/job.111
[42] Lee, H., Cummings, G.G. (2008). Factors influencing job satisfaction of front line nurse managers: A systematic review. Journal of Nursing Management, 16(7): 768-783. https://doi.org/10.1111/j.1365-2834.2008.00879.x
[43] Greenslade, J.H., Jimmieson, N.L. (2007). Distinguishing between task and contextual performance for nurses: Development of a job performance scale. Journal of Advanced Nursing, 58(6): 602-611. https://doi.org/10.1111/j.1365-2648.2007.04256.x
[44] Schwirian, P.M. (1978). Evaluating the performance of nurses. Nursing Research, 27(6): 347-350. https://doi.org/10.1097/00006199-197811000-00004
[45] DrachZahavy, A. (2004). Toward a multidimensional construct of social support: Implications of provider's self-reliance and request characteristics. Journal of Applied Social Psychology, 34(7): 1395-1420. https://doi.org/10.1111/j.1559-1816.2004.tb02012.x
[46] Fort, A.L., Voltero, L. (2004). Factors affecting the performance of maternal health care providers in Armenia. Human Resources for Health, 2(1). https://doi.org/10.1186/1478-4491-2-8
[47] Rose, R.C., Kumar, N., Pak, O.G. (2011). The effect of organizational learning on organizational commitment, job satisfaction and work performance. Journal of Applied Business Research, 25(6): 55-66. https://doi.org/10.19030/jabr.v25i6.995
[48] Kazemipour, F., Mohamad Amin, S., Pourseidi, B. (2012). Relationship between workplace spirituality and organizational citizenship behavior among nurses through mediation of affective organizational commitment. Journal of Nursing Scholarship, 44(3): 302-310. https://doi.org/10.1111/j.1547-5069.2012.01456.x
[49] Noh, G.M., Yoo, M.S. (2016). Effects of workplace spirituality and organizational citizenship behavior on nursing performance. Journal of Korean Academy of Nursing Administration, 22(3): 251. https://doi.org/10.11111/jkana.2016.22.3.251
[50] Riketta, M. (2002). Attitudinal organizational commitment and job performance: A meta-analysis. Journal of Organizational Behavior, 23(3): 257-266. https://doi.org/10.1002/job.141
[51] McGrath, R.G., MacMillan, I.C. (2000). The entrepreneurial mindset: Strategies for Continuously Creating Opportunity in an age of Uncertainty. Harvard Business Press.
[52] Organ, D.W., Ryan, K. (1995). A meta-analytic review of attitudinal and dispositional predictors of organizational citizenship behavior. Personnel Psychology, 48(4): 775-802. https://doi.org/10.1111/j.1744-6570.1995.tb01781.x
[53] Saunders, M., Lewis, P., Thornhill, A. (2009). Research Methods for Business Students. Prentice Hall.
[54] Joshi, A., Kale, S., Chandel, S., Pal, D. (2015). Likert scale: Explored and explained. British Journal of Applied Science & Technology, 7(4): 396-403. https://doi.org/10.9734/bjast/2015/14975
[55] Hair, J.F., Ringle, C.M., Gudergan, S.P., Fischer, A., Nitzl, C., Menictas, C. (2018). Partial least squares structural equation modeling-based discrete choice modeling: An illustration in modeling retailer choice. Business Research, 12(1): 115-142. https://doi.org/10.1007/s40685-018-0072-4
[56] Jöreskog, K.G., Sörbom, D. (1996). LISREL 8: User’s Reference Guide. Scientific Software International.
[57] Sugiyono. (2014). Educational Research Methods Quantitative, Qualitative, and R&D Approaches. Alfa Beta, Bandung.
[58] Henseler, J., Ringle, C.M., Sarstedt, M. (2014). A new criterion for assessing discriminant validity in variance-based structural equation modeling. Journal of the Academy of Marketing Science, 43(1): 115-135. https://doi.org/10.1007/s11747-014-0403-8
[59] Hair, J.F., Hult, G.T.M., Ringle, C.M., Sarstedt, M. (2017). A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM) (2nd ed.). SAGE Publications.
[60] Gagnon, M.P., Payne-Gagnon, J., Fortin, J.P., Paré, G., Côté, J., Courcy, F. (2015). A learning organization in the service of knowledge management among nurses: A case study. International Journal of Information Management, 35(5): 636-642. https://doi.org/10.1016/j.ijinfomgt.2015.05.001
[61] Calisir, F., Altin Gumussoy, C., Guzelsoy, E. (2013). Impacts of learning orientation on product innovation performance. The Learning Organization, 20(3): 176-194. https://doi.org/10.1108/09696471311328442
[62] Sung Jun Jo, Joo, B.K. (2011). Knowledge sharing: The influences of learning organization culture, organizational commitment, and organizational citizenship behaviors. Journal of Leadership & Organizational Studies, 18(3): 353-364. https://doi.org/10.1177/1548051811405208
[63] Xanthopoulou, D., Bakker, A.B., Demerouti, E., Schaufeli, W.B. (2009). Work engagement and financial returns: A diary study on the role of job and personal resources. Journal of Occupational and Organizational Psychology, 82(1): 183-200. https://doi.org/10.1348/096317908x285633
[64] Somech, A., Drach-Zahavy, A. (2004). Exploring organizational citizenship behaviour from an organizational perspective: The relationship between organizational learning and organizational citizenship behaviour. Journal of Occupational and Organizational Psychology, 77(3): 281-298. https://doi.org/10.1348/0963179041752709
[65] Islam, T., Khan, S.U.R., Ahmad, U.N.U., Ahmed, I. (2014). Exploring the relationship between POS, OLC, job satisfaction and OCB. Procedia - Social and Behavioral Sciences, 114: 164-169. https://doi.org/10.1016/j.sbspro.2013.12.678
[66] Cascio, W.F., Boudreau, J.W. (2016). The search for global competence: From international HR to talent management. Journal of World Business, 51(1): 103-114. https://doi.org/10.1016/j.jwb.2015.10.002
[67] May, T.Y., Korczynski, M., Frenkel, S.J. (2002). Organizational and occupational commitment: Knowledge workers in large corporations. Journal of Management Studies, 39(6): 775-801. https://doi.org/10.1111/1467-6486.00311
[68] Xie, D. (2005). Exploring organizational learning culture, job satisfaction, motivation to learn, organizational commitment, and internal service quality in a sport organization. The Ohio State University.
[69] Suifan, T.S., Allouzi, R.A.R. (2018). Investigating the impact of a learning organization on organizational performance: The mediating role of organizational commitment. International Business Management, 12: 230-237.
[70] Kwan, H.K., Mao, Y. (2011). The role of citizenship behavior in personal learning and work-family enrichment. Frontiers of Business Research in China, 5(1): 96-120. https://doi.org/10.1007/s11782-011-0123-6
[71] Chun, J.S., Shin, Y., Choi, J.N., Kim, M.S. (2011). How does corporate ethics contribute to firm financial performance? Journal of Management, 39(4): 853-877. https://doi.org/10.1177/0149206311419662