Daoudi Tamoud Mounya*![]() | Hocine Mohamed
| Hocine Mohamed![]() | Cherfaoui Dounia
| Cherfaoui Dounia![]()
© 2024 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
This study investigates the impacts of the COVID-19 pandemic on urban planning to develop an urban resilience strategy. The vulnerability assessment of Algiers to COVID-19 seeks to develop a correlation between the pandemics’ global systemic impacts and Algiers' local urban potential. This research outlines the methodological approach of the Group Analysis Method (GAM), the multi-criteria decision analysis method (MCDA), and the qualitative analytical reading method (SFPO) - Successes, Failures, Potential, and Obstacles. These methods allowed us to build the Restricted Targeted Self-Audit (RTSA) and finally the planning framework. This study yields two distinct types of results: theoretical findings related to the expansion of the urban sustainability model and the empirical findings triggered by the issue of pandemic resilience. The results of this study aim to enhance residents’ adaptation to major urban risks through proactive urban planning actions. This will help prevent a critical crisis for the city and its inhabitants in the event of a future pandemic.
Algiers, COVID-19, pandemic risk, resilience, urban health planning, vulnerability assessment
Cities are recognised as the most vulnerable human settlements to pandemics and bear significant responsibility for their propagation, given the extensive human, societal, environmental, economic, and political consequences. Within urban areas, the emergence of infection clusters can be attributed to various factors, notably the density of human activity, population mobility, toxic waste discharge, poverty, inadequate hygiene, insufficient healthcare services, and specific microclimatic conditions. Lévy [1] succinctly captured this interconnected association: "The question of health is a major determinant of urban planning".
The importance of health in the urban environment resurfaced with the initiation of the Healthy Cities Programmed by the World Health Organisation WHO in 1986 [2], which perceives the city as a living organism. Subsequently, in 2015, the 17 UN-SDGs (United Nations Sustainable Development Goals 2030) significantly reinforced the recognition of health issues.
Sustainable urban planning has focused on multiple systemic challenges, overshadowing the importance of health within urban context, despite major risk concerns [3]. In contrast, early urban theories (hygienist, culturalist, functionalist and progressive) aimed to devise urban models that addressed the issues of city health and cleanliness through initiatives such as Haussmann’s restructuring, Howard’s garden city model, Garner’s radial cities, Cerda’s grid plan, and the works of Le Corbusier, Tange, Wright, and others.
The three major urban transformations—from the pathogenic city of the 19th century to the polluted city of the 20th century and now to the ecological city of the 21st century—are gradually paving the way for a fourth shift in urban planning. This new shift prioritises human health and well-being, focusing on the development of a postmodern sustainable city and a post-COVID-19 resilient city, placing these concerns at the forefront of contemporary urban strategies.
The devastating impacts of pandemics, combined with climate change, and ecological, economic, social and managerial crises, require urgent decisions to be taken at both global and local levels [4-6]. Hossain stated, “the current COVID-19 pandemic made the global economy and trade slow down while the ill effects are realised and perceived at a regional and local level” [7]. The epidemic outbreak in Bangladesh highlighted the vulnerability of the health and healthcare systems [8] and financial scarcity for public health management, similar to other developing countries, due to their uneven society, underdeveloped healthcare systems, and prevalent poverty [9]. Algiers is also quite vulnerable to pandemics [10] and climate change [11]. In this context, urban planning, which is responsible for the development and management of urban spaces, plays a key role to play. Urban planning can and must help to encounter the challenges posed by a systemic crisis of this scale “where the latter underlines self-sufficiency, entrepreneurship, and innovations through transformation and redefining service delivery and core activities with improving the existing services and supplying news services” [12].
The Organisation for Economic Co-operation and Development OECD (2020) highlighted those major cities worldwide, as pandemic epicentres, have adopted nearly identical measures to fight the virus. It asserts that urban density is not the primary cause of vulnerability; rather, vulnerability is primarily influenced by organisational choices, lifestyles, work patterns, and travel behaviours. In contrast, in Africa, populations have experienced a lower COVID-19 impact, accelerated urbanisation poses a significant risk factor. When combined with inadequate urban planning, limited employment opportunities, the prevalence of informality, inadequate access to healthcare facilities, low levels of digitalisation and, food insecurity, poverty, and social inequalities amplify cities’ vulnerability in terms of loss of local development capacity. Ultimately, COVID-19 has had similar effects worldwide, irrespective of the level of development [7].
In various UN reports, a consistent observation is made: "There is an urgent need to re-evaluate and transform cities to address the realities of COVID-19 and potential future pandemics while striving for better recovery through the development of more resilient, inclusive, and sustainable urban environments" [13]. Urban planners have traditionally been proactive in addressing the challenges associated with extreme events. However, in Algeria, significant urban restructuring is largely overlooked despite, its critical importance [14]. Public authorities hesitate in implementing such measures, possibly because of their complexity and the challenges associated with their execution. Nonetheless, these actions have the potential to cause positive outcomes and contribute to urban rejuvenation in cities. “So it is necessary to transform the challenges into opportunities through triggering reform and innovations in governance” [7].
This paper investigates the impacts of the COVID-19 pandemic on urban planning to formulate an urban resilience strategy that encompasses restructuring, reorganisation, requalification, and reinvention of the city.
In this research, we focus on Algiers, composed of 57 municipalities (809 km²), with a population of more than 3.2 million and a population of more than 6.5 million in the metropolitan area [15]. The governing tools employed for the city's management date back to the 1990 urban planning reform, and while some adjustments have been made since then, these tools remain largely outdated. Algiers has a progressive Master Plan for Development and Urban Planning (PDAU 2035) that prioritises sustainability [16]. This plan has created a realisation of the necessity to align with the global approach to sustainable development [17]. While ongoing reforms aim to modernise urban planning tools and instruments, the pandemic has brought new urban needs and vulnerabilities that were previously underestimated and now demand consideration. Consequently, understanding the pandemic's effects facilitates the identification of appropriate urban resilience factors, which can guide strategic actions for implementation by public authorities.
This study aims to identify the performance and vulnerability factors of Algiers’ urban ecosystem to inform strategies for improving its resilience against substantial health risks. Likewise, the search identifies critical needs that have emerged during the COVID-19 pandemic. Our research on local urban vulnerability will employ mainly the Group Analysis Method (GAM) combined with the multi-criteria decision analysis method (MCDA) and, the qualitative analytical reading method (SFPO - Successes, Failures, Potential, and Obstacles). The crucial goal is to develop a RTSA dedicated to the city's internal assessment process and ultimately improve the capacity to answer health crises.
MCDA Analysis is a comprehensive, systemic and structured approach for evaluating and prioritising alternative based on multiple and conflicting criteria. In terms of resilience, MCDA planning studies will aid us in assessing the vulnerability of the Algiers population to the pandemic. Particularly by defining the problem, identifying, and weighting criteria, and ranking and communicating results [18]. It will allow us to set a more evidence-based approach to COVID-19 vulnerability assessment and contribute to more effective pandemic management [19]. For analytical purposes, the SFPO method based on collective learning [20] was very helpful to implement a prospective strategy.
International organisations like UNDP and UN-Habitat advocate for the development of a city’s internal assessment process to evaluate its ability to withstand, adapt to, and recover from disruptions like pandemics. RTSA empirical approach focuses on critical systems or areas, involves local stakeholders and experts, and provide actionable recommendations for city leaders. By conducting an RTSA, cities can better understand their resilience, prioritise interventions, and develop specific strategies to enhance their ability to manage disruptions. This approach complements larger assessments by offering a more focused and context-specific evaluation of urban resilience management.
2.1 GAM
The MAG, originating from Belgium [20, 21], stands at the core of our methodological approach. This qualitative analysis method is selected for its flexibility, allowing experts to navigate the uncertainties that arise from a lack of quantitative data or the need to rely on approximations. The scarcity of specific data, such as the number of hospital patients per municipality, the capacity limits of local health facilities, and the broader impacts on employment, education, and environmental conditions, poses significant challenges in fully assessing the consequences of the containment measures. These challenges extend to understanding critical factors like job losses, compliance with public health restrictions, environmental repercussions, mental health concerns, and variations in crime rates, all of which are essential for comprehensively grasping the local effects of the pandemic.
The key advantage of GAM lies in its reliance on experts with proven experience because they can detect alarming situations effectively. In GAM, researchers present the group with targeted questions derived from a predefined matrix. The experts then assess the level of vulnerability of the system under examination by considering various scenarios presented in the matrix. They drew upon expertise in urban planning and experience with the COVID-19 pandemic to perform this assessment.
2.1.1 Performing group analysis method
The entire group of (8) eight experts participated in the analysis through RTSA. The experts actively participated in the audit from the outset, with consultation and result analysis conducted digitally via Google Meet. During this meeting, the main findings were ratified. Subsequently, the collected data were deliberated upon to synthesise the assessments and steer urban efforts towards enhancing resilience and facilitating the reform of urban planning tools in Algiers. The digital consultation spanned 11 months. Subsequently, we analysed the outcomes, and a group meeting was held via Google Meet.
2.1.2 Profile of the participants
The consultation group comprised architects-urbanists with professional experience and teachers-researchers in urban planning, all of whom were members of the QUEDD Team at the VUDD Laboratory of the EPAU in Algiers. They reside in the provinces of Algiers and Blida, and they have contact persons with various profiles (trade, administration, logistics, health services, education, and civil defence). The age of experts is mostly in the range 30-50 years (63%).
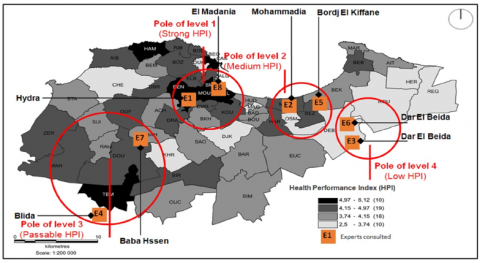
The participants came from seven municipalities in Algiers. The spatial distribution of residence places of the households consulted represents the four poles of health performance at different levels, identified by the HPI (Health Performance Index) [21] (Figure 1). HPI draws for Algiers the most efficient municipalities, but also shows that, need the urgent implementation of a strategy prospective improvement of health performance by setting up resilient urban health planning to pandemics.
2.1.3 Basis of assessment
We based the assessment on three main data sources: PDAU 2016 data [18]; “Baromètre des performances locales d’Alger” 2015 [22]; PhD research project [10]. Several other sources we quote 3: (1) thematic reference systems, such as WHO reports, state institutions (Ministries of Health, Interior and Foreign Affairs), (2) the Algerian press (quotidiens El Watan, Liberté), media (TV Canal Algérie, Algerian radio Chaîne III and social media (FB, YouTube); and (3) the personal experience of the participants.
Figure 1. Location of the homes of experts consulted
2.2 Phases of GAM analysis
The GAM process can be summarised in four phases, as follows: The preliminary phase establishes a contextual database. The preparatory phase involves setting up a theoretical model of resilient urban ecosystem, selecting urban resilience characteristics, and establishing the vulnerability assessment framework MCDA analysis for COVID-19-oriented RTSA. The operational phase identifies the expert witness group involved in the GAM analysis, discusses the findings, and visualises the results. The analytical phase using the SFPO method identifies the current city’s current weaknesses and provides recommendations.
2.2.1 The preliminary phase
The preliminary phase of this study evaluates health performance in Algiers by identifying key indicators for urban health performance/vulnerability. These indicators, derived from the WHO City Health Programme’s structural analysis, include the availability and proximity of health facilities, access to nature, and proximity to health hazards. Additionally, this phase uncovers essential qualities necessary for assessing health performance, such as: Autonomy: Functioning, organization, management, planning, and spatial use. Proximity and Accessibility: Access to basic and specialized facilities, and nature. Protection: Safeguards against major urban risks.
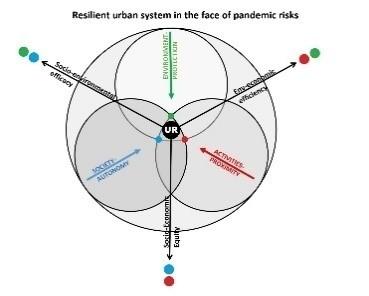
Figure 2. Adopted model of resilient urban sustainability to pandemic risks
Recognising that a city cannot claim to be sustainable if it lacks resilience [6, 23], we establish a conceptual model of urban health resilience that, delves deeper than the traditional urban sustainability model (Figure 2). This model serves as the basis for constructing a COVID-19-oriented assessment matrix (Table 1).
Table 1. Assessment matrix for system vulnerability factors
|
|
Factor Xn(1-3) |
|
|
||||||
|
|
Variable Ym(1-4) |
|
|||||||
|
|
Situations observed to considerate Z (a-d) |
Appreciation N (1-5) |
Corresponding additional situations |
score per situation (1-5) |
|||||
|
|
1 |
2 |
3 |
4 |
5 |
||||
|
a) |
|
x |
|
|
|
|
|
1 |
|
|
b) |
|
|
|
x |
|
|
|
3 |
|
|
c) |
|
|
|
x |
|
|
|
3 |
|
|
d) |
|
|
|
|
X |
|
|
4 |
|
|
|
|
1 |
|
6 |
4 |
|
Total points per variable |
Nv=∑Nz(a-d)/(4-20) |
|
|
|
|
Total points per factor |
NF=∑Nv(1-4)/(16-80) |
||||||
|
|
|
Total points per factor and expert (global square per expert) |
NE=∑NF(1-3)/(48-240) |
||||||
|
|
|
Total global points per factor |
NGF=8x[∑NF(1-3)/(48-240)] NGF=N/(128-640) |
||||||
|
Qualitative scale of the overall assessment of variables |
Cumulative score range (8 experts) |
||||||||
|
Average relative performance |
> 96 (Scale average) |
||||||||
|
Weak performance |
90 – 96 |
||||||||
|
Vulnerability threshold |
90 |
||||||||
|
Health vulnerability |
˂ 90 |
||||||||
Table 2. Criteria for assessing the model's components
|
Vulnerability Factors |
Target Areas and Characteristics |
Components and Situations Assessed |
|
1. Autonomy |
1.1. functional adaptation (Flexibility, adaptability) |
Technical infrastructure, Buildings, Roads and green and open public spaces, Local management and organization |
|
1.2. decentralization (Availability, integration) |
Information and communication, Local production, Sharing of local resources, intermunicipality |
|
|
1.3. consultation & dialogue (co-ordination, involvement) |
Urban planning, Urban programming, Urban development, Operational management |
|
|
1.4. management of local vital resources (capacity and self-sufficiency) |
Land, Natural Resources (water, energy, food, biodiversity), Human Resources, Financial Resources |
|
|
2. Proximity |
2.1. exposure to health risk compactness and respect for development rules |
Urban density, Green density, Roads and other networks, Facilities and nerve centres (hospitals, stations, markets, schools and high schools, town halls, post and telecommunications, drinking water and energy distribution centre) |
|
2.2. facilities and services Accessibility, innovative offering |
Complements of sanitary facilities, Basic services, Education and Recreation, Information and communication |
|
|
2.3. local urban resources Diversification, specialization |
Public land for special developments, Biodiversity areas, health logistics, Employment and training |
|
|
2.4. mobility Interaction, distancing |
Information exchange, mobility management, Air and maritime transport, Administrative organization |
|
|
3. Protection |
3.1. territory securing closing of circuits, accessibility |
The local economy, Adapted housing, Facilities and infrastructure for accessibility and supply, Food security |
|
3.2. medical evacuation and hygiene closure of circuits, accessibility |
Evacuation networks and logistics, Reception areas, Sanitation equipment, Communication and supplies |
|
|
3.3. Sanitary isolation Protection, isolation |
Local vulnerability profiles, Architectural and urban conversion/polyvalence (housing, facilities), Communication, Emergency supplies |
|
|
3.4. concomitant risk management Foresight, synchronization |
Database, Urban planning tools, Emergency Management, Aid to the population |
2.2.2 Preparatory phase
The preparatory phase of the COVID-19-oriented assessment provides the theoretical foundation for the analysis. The assessment matrix uses the Multi-Criteria Decision Analysis (MCDA) method, integrating systemic components that emphasises three key factors crucial to local health performance: local autonomy in functioning, proximity to vital activities, and protection against risks. It also outlines the corresponding urban planning areas and desired characteristics.
2.2.3 The operational phase
The operational phase of the COVID-19-oriented assessment entails the following tasks: (i) setting up assessment grids following GAM Analysis; (ii) inviting a group of experts to participate in the assessment; (iii) conducting discussions and analysing the results:
The assessment matrix framework is presented in Table 2 above, comprising 3 thematic grids, 12 variables, and 48 criteria. The urban resilience approach chosen centres on vulnerability factors. Each grid corresponds to a factor previously identified as relevant in a threatening situation, previously (Figure 2). Four variables characterise each factor, serving as situations or criteria:
Autonomy: Functional adaptation, Decentralisation, Dialogue, Resource management;
Proximity: Risk exposure, Facilities and services, urban resources, Mobility;
Protection: Security, Evacuation, Sanitary isolation, Risk management.
The method involves selecting a box on a scale of 1 to 5 for each situation encountered online, positioned on the left and right sides of the rating scale (refer to Figure 3). This process allows the expression of an opinion on which of the two situations more accurately describes the observed performance of the specific criterion.
The number (1 or 2) is chosen if the situation on the left is deemed more appropriate, (3) if both situations are equally significant, and (4 or 5) if the situation on the right is considered more fitting. In cases in which both situations appear equally valid and complementary, it is recommended to weigh them based on their importance in intensifying the current health vulnerability of the Algiers urban system.
The group involved in the assessment consisted of eight (8) experts, forming participatory subsystems. This group is considered competent due to their shared experience of living under the COVID-19 pandemic threat. They encountered the same territorial, geo-economic, and climatic conditions and faced similar health policy restrictions during the same period.
The presence of diverse opinions, which are valuable, may arise from differences in personal, family, or professional situations, variations in exposure or vulnerability to threats, and individual sociodemographic profiles.
The analytical phase with SFPO method permitted to identify current weaknesses and provides recommendations for actions necessary to achieve a desirable level of local urban resilience.
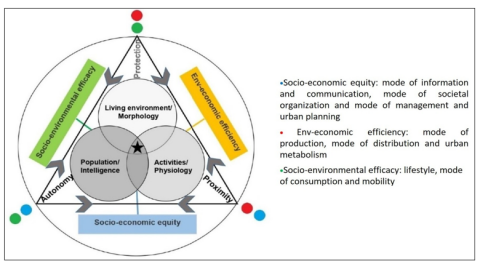
Figure 3. Developed model of the resilient urban ecosystem, facing the risks of a pandemic
This study produces two distinct categories of results. The first category comprises theoretical findings that contribute to the development of urban sustainability model in response to the challenges of pandemic resilience. These theoretical results facilitate the assessment of Algiers’ urban vulnerability during the COVID-19 pandemic. The second type of result pertains to empirical findings, associated with RTSA.
3.1 Theoretical results of the founding concepts of the RTSA
The preparatory phase of the study revealed the possibility of introducing perspective on resilient sustainable urban ecosystems model. This proposed organic approach introduces an additional interrelationship between the fundamental principles of sustainability, namely equity, efficiency, and effectiveness (Figure 3).
3.1.1 Resilience factors used
Typically, these principles underlie all sustainability indicator frameworks derived from the primary triangular model, which encompasses society, environment, and economy. This study emphasised three key resilience factors: autonomy, proximity, and protection (Table 2).
Protection against risks falls within the scope of "morphology" or the interplay between effectiveness and efficiency concerning the need for safeguarding, which is associated with the notion of "liveability". In the context of local performance assessment, environmental efficiency and socioeconomic effectiveness have distinct definitions. Environmental efficiency, specifically, refers to the municipality's capacity to address climate change, manage resources, and preserve environmental quality. On the other hand, socioeconomic effectiveness gauges the municipality's ability to cater to local socioeconomic demands by promoting crucial developmental activities [24].
When any single component (be it an individual, environment, or resource) lacks protection, the entire system suffers an impact. Resilient urban planning must offer tools to manage major risks in an urban environment. These tools must be capable of planning, developing, and managing a city to ensure the territory's security and the preservation of vital resources. Additionally, they must facilitate evacuation, sanitary isolation, and the management of concurrent risks. Proactive measures are required to ensure the protection of the population.
The Proximity of vital activities falls within the "physiology" dimension or equity/efficiency interaction. In this context, equity means equal access to services that the municipality can provide for all its inhabitants. Beyond the connotation of "viable," it concerns living and not just surviving, even in the presence of restrictive measures imposed by public authorities.
Resilient urban planning must address diverse needs to ensure the long-term sustainability of a city. It is essential to find solutions for urban density and the sustainability of local resources like water, energy, and nature while, also fostering a local circular economy. Additionally, it is necessary to facilitate local employment opportunities and provide adequate urban facilities and services to ensure the availability of information, training, and fair communication at the local level.
Finally, the local Autonomy of functioning is associated with the "intelligence" dimension, which reflects the connotation of "reliability" and the interaction of equity and effectiveness. The municipality must to sustain life while considering the changes brought about by the pandemic, such as communication modes, societal organisation, management, and urban planning. To achieve this objective, it must mobilise all available: technical, technological, logistical, financial, regulatory and human, resources. To ensure local autonomy, urban intelligence must encompass adaptation, decentralization, consultation, and management. These elements require a swift operational response to ensure the flexibility of networks and infrastructures, the adaptive use of buildings, the multi-functionality of green and open spaces, the integration of production activities at the local level and, the pooling of financial and human resources. An inter-municipal approach, citizen participation, and transparent monitoring methods are also crucial.
3.1.2 Pandemic and resilient urban planning
The pandemic has induced changes in lifestyles, work, consumption, production, distribution, and mobility. To handle these changes, it was necessary to rebuild buildings and develop the flexibility of networks and infrastructures. Local-level integration of production activities was necessary, with natural, financial, and human resources requiring consolidation through an inter-municipal approach. Citizen participation and transparent local monitoring are also significant factors in ensuring rapid operational response to major risks in urban areas. Such experimentation must adhere to laws and socio-professional ethics, as it is crucial to ensure the operational nature of all other factors of urban health resilience. In fact, this study’s limited scope limits it from exploring the prospect of resilient urban planning, which is something we seek to enhance in Algiers.
3.2 Empirical results related to RTSA
3.2.1 Results of audit
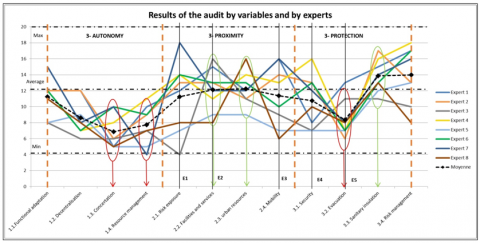
It is crucial to emphasise that this study on Algiers’ vulnerability to COVID-19 does not pertain to pandemic management measures formulated and implemented by public authorities (e.g., restrictions, closures, curfews, healthcare methods, treatments, etc.). Its sole and exclusive objective is to assess urban development, management, and planning criteria that contribute (or do not contribute) to the health resilience of the urban system in Algiers. The qualitative assessment results are presented as a line graph (Figure 4).
Figure 4. Results of the audit by variables and by experts
A direct examination of these findings reveals several interesting observations:
Five of eight experts (5/8) expressed dissatisfaction with urban health performance during the COVID-19 pandemic. Their overall rating was below average (144 points out of 240 is considered the cut-off point for shifting from relative performance to vulnerability).
Among the twelve variables analysed, five strongly contribute to Algiers’ urban vulnerability (Decentralisation, Consultation, Management of Vital Resources, Security, and Evacuation). Conversely, the remaining four variables exhibit rather optimistic results (Equipment and services, urban resources, isolation, and urban risk management). However, a consensus is observed for the three (3) variables considered to have the most significant impact on health vulnerability: Consultation, Management of vital resources, and Evacuation. However, this initial analysis is not sufficient as it does not allow for comparing the obtained values, establishing a hierarchy of priorities for the three studied factors, or formulating clear recommendations for resilient urban planning. Consequently, we chose the therapeutic model of urban resilience, which aims to achieve a set of systemic goals to cure the patient while avoiding unwanted side effects. This approach differs from the ballistic model, which does not consider the entire organism [22] cited in study of Berezowska-Azzag [25]. This choice is in line with the previously described organic model of urban resilience.
3.2.2 Results of the SFPO method
The SFPO method is based on collective learning and combines quantitative and qualitative systemic approaches. It matches experiences, in the left-hand column of the RTSA assessment grid, with the experts' hopes (right-hand column) expressed in the analysis [20]. An effective way to check the degree of consensus between the experts in the group on the nature of the actions to be proposed. Although the SFPO method may reveal conflict of perspective, selecting an expert panel is important [20]. The study could be conducted using a grid of MCDA indicators to measure certain quantitative or qualitative results, allowing for a more in-depth analysis.
The perception of the 48 situations for the 12 variables analysed by the experts in the assessment contributes to the creation of the SFPO assessment sheets (see appendix). These sheets led to the visualisation of the findings, summarised in Table 3.
Table 3. SFPO analysis sheet template
|
Variable Yn(1-4) of Factor Xn(1-3) (with Its Desired Characteristics) |
||||
|
|
Retrospective Gaze |
PROSPECTIVE Gaze |
||
|
Positive aspects identified |
Success: |
•Positive situations and observed successes •Objectives achieved •Strengths •Membership-building activities •Promising activities |
Potentialities: |
•Success to deepen •Transformed failures •Ideas, wishes, assets to exploit •Untapped capacities •New challenges |
|
Negative aspects identified |
Failures: |
•Endogenous difficulties and weak points •Oppressive situations •Double Constraints •Impasses and harmful effects •Effective drifts |
Obstacles: |
•Disabilities, oppositions, blockages •Actor resistance •Unfavourable exogenous conditions •Objective limits •Possible drifts |
Table 4. Identification of needs according to the SFPO analysis by health planning intervention areas
|
Area of Action for Health Planning |
Factors of Urban Resilience to Health and Pandemic Risks |
||||
|
Autonomy |
Proximity |
Protection |
|||
|
Diagnosis of the health vulnerability of “issues” (local health profile, local vulnerability index, atlas of exposure to major risks) + Human, social, economic, environmental, urban construction and infrastructure, managerial, political and institutional issues |
Algiers: Towards a healthy, revitalised and resilient city |
•Availability of vital resources (water, energy, food, telecommunications); •Availability of facilities (health, education, sport and leisure, culture, shopping, administration); •Availability and efficiency of urban services (sanitation, supplies, disposal, transportation); •Compliance with urban carrying capacity (security density, biodiversity and ecological services) Green index; •Equipment: emergency logistics (heliport, municipal logistics park, teleport, maintenance facilities); •Digitisation of databases; Behaviour guides and local risk exposure atlases. |
•Accessibility to basic facilities within a maximum 15-minute walk; •Accessibility for emergency services (penetration and access for civil protection, ambulances); •Multi-purpose and multi-modal parking capacity; •Proximity to mass transit stops; Access to nature; •Short food supply circuits and their ancillary spaces (delivery/ordering boxes) •Possibility of local employment, teleworking, e-learning; •Access to information; •Accessibility to multi-service public places (recharging batteries, paying bills, sending mail, etc.). |
•Location of evacuation areas and emergency relay platforms; •Identification of evacuation routes; •Compliance with planning standards for sanitary and civil protection facilities; •Integration of technical emergency networks in housing areas (fire-fighting network and hydrants, lifting equipment); •Integration of local energy production facilities (in the event of a blackout); •Elimination of sources of health, noise, and odour nuisance; •Technological development and robotisation; •Training in new urban professions. |
|
|
Resilience strategy |
•Identification of exogenous pressures (climate, health, economic, social, and food crises) and endogenous pressures (unemployment, social and territorial inequalities, housing crisis, lack of land available for development, pollution, obstacles to mobility, bureaucracy, fall in local finances, low level of digitisation, etc.) •SWOT analysis and precariousness of resilience issues; •Urban health resilience scenarios; •Local Agenda 21, Action Plan. |
||||
|
Urban planning and programming |
•Resilient urban planning (urban form, urban carrying capacity, residential safety density, vital facilities grid, infrastructure density, local urban metabolism); •Thematic urban projects linked to local issues (climate adaptation, healthy cities, etc.); •Local urban resilience master plans; •Other tools (classification, labelling). |
•Urban planning at limit states (Carrying capacity thresholds, carbon footprint, biodiversity index, vegetation index); •Participatory planning; •Urban development projects (Iterative, transversal, flexible and negotiable) and urban symbioses, industrial and ecological symbioses. |
•Local plans for protection against major risks (health, natural, technological, climatic); •Local inter-municipal solidarity charters; •Project contracts (equipment, structure, and protection facilities). |
||
|
Urban development design |
•Decentralised/separate technical infrastructure network (rainwater, renewable energy, sewerage, telecommunications) (Production and storage/distribution/collection/local pre-treatment); •Revitalisation/regeneration of local land, possible re-parcelling; •Local collection and treatment of household waste (Automation, robotisation, 4Rs and circular economy); •Functional versatility of buildings (reconversion, flexibility of use) (housing, large facilities, office buildings); •Green networks, greening and local biodiversity corridors (sport, recreation, sanitation, carbon reduction, food production); •Road networks that can be adapted to the needs of soft traffic (30 km/h zones) and emergency traffic (freed-up areas); •Plots set aside for flexible collective activities (co-working, co-production, co-processing, communication / information, other). |
•Development of natural areas: gardens, parks (accessible within 10 minutes on foot); •Integration of local agriculture (horizontal, vertical), local food production/processing/security; •Rainwater storage (retention basins, water tanks); •Local treatment of grey water; Integration of renewable energy production equipment (photovoltaic panels, geothermal energy, sensors, urban wind turbines, methanation); •Improved accessibility (intelligent parking, delivery points, waste collection points, heliport, secure monorail overhead circuits, de-densification, curing of lots, etc.). |
•Health facilities (P4 laboratory, medical equipment storage centre, emergency aid points/boxes, public rest areas, health/isolation accommodation, physiotherapy and psychotherapy centres); •The municipality's logistical facilities (municipal fleet of emergency vehicles and equipment. Location of emergency reception sites, heliport, storage of vital foodstuffs); •Adaptable road infrastructure, evacuation networks and secure TCSP corridors, buffer zones (pollution, noise pollution, health protection, explosion, fire); •Perimeters protecting nerve centres from health, natural and technological risks; •Soft traffic and pedestrian networks; •Designation and development of public relay/rescue areas (equipped medical platforms, assembly/isolation lights) Relocation/conversion/technological modernisation of health-endangering facilities. |
||
|
Project processing and monitoring |
•Action plan, planning, budgeting, co-financing of health resilience projects; •Monitoring of ecosystemic impacts during implementation; •HSE assessment (worksites), HQE (projects) and City-Health certification/labelling; •PPP partnership, assessment of public action. |
||||
|
Monitoring and management of urban development |
•Town planning agencies and specialised local units (databases, impact analysis, special studies, technological development, continuing training for managers) •Local observatory for resilient development (Alerts when it reaches local thresholds of Resilience capacity) |
•Monitoring quality of life and quality of the environment; •Land and financial prospecting; •Territorial marketing of resilience qualities (conceptual, technical, and technological innovation); •Intelligent, participatory and partnership-based management (organisation, institutional structure, assessment techniques, therapeutic focus forum, expertise, training, inclusive innovation workshop, think-tank, experience sharing, etc.). |
|||
The study’s objective is to find ways of revitalising urban planning for the future, considering that the city of Algiers, like many others, is facing multiple crises [26-29]. The results obtained in this study contribute to the literature review. The pressure exerted by these crises has necessitated a search for solutions to ensure the urban resilience and sustainability of the cities.
This allows the identification of shortcomings and designates the parameters on which action should be taken (Table 4). We identified “Needs” in the areas of cross-sectoral consultation/citizen participation and the management of vital resources to enhance urban resilience.
These findings led to the revision of legal and regulatory texts to integrate health risk, the addition of urban planning tools with the theme of health resilience, the implementation of a warning system on the use of land, natural, human, and financial resources, the structural reorganization of local authorities and local management by projects (Table 4). This discrepancy should be addressed in current Algiers’s PDAU, which aims for a horizon of 2035 but acknowledges the need for regular plan updates. The SFPO prospective analysis revealed an imbalance between hopes (existing needs and potentialities) and observations (obstacles to be overcome), requiring a strategic approach that takes time to balance (Table 5).
Table 5. Obstacles to be removed according to the SEPO analysis by areas of public action
|
Areas of Public Action |
Factors in Urban Resilience to Health and Pandemic Risks |
||||
|
Autonomy |
Proximity |
Protection |
|||
|
Adaptation / compliment/ Revision of legislation / regulations |
Algiers: Towards a healthy, revitalised and resilient city |
•Municipal, provincial and city laws; Inter-municipal project contracts (within the perimeter of the Algiers province to ensure autonomy in the event of territory closure); •Local partnership, consultation and citizen participation •Functional reconversion procedures; •Procedures for decentralising technical infrastructure networks (renewable energy, sanitation, waste collection and treatment). |
•Legislation relating to town and country planning, health, environment, waste, energy, new towns and protected sites; •Programming standards and urban easements. |
•Legislation relating to health, climate, town and country planning, protected sites, environment, biodiversity, air quality, waste, water, etc.; •Insurance (health risks, acceptability thresholds, disaster decrees, etc.) |
|
|
Creation / reorganisation of organisations and institutions |
•Training institute for cities and major risks; •Local town planning agency; •Local environment and resilient development observatory •Health monitoring units (neighbourhoods). |
Creation of themed collaborative workshops. Collaboration between municipalities and schools |
Urban management by project or objective (not by sector) Reorganisation of municipalities (thematic committees) |
||
|
Local funding |
•Public procurement code •Local development fund •PPP Participation |
•Encouraging local SMI/SMEs, micro-businesses and start-ups; •Innovative local partnerships. |
•Encouraging local SMI/SMEs and micro-enterprises |
||
|
Complementary planning tools |
•Urban planning grids; •Charter for public spaces and the environment; •Local Agenda 21; •Urban Health Project; •Circular economy guide. |
•Local climate and energy plan; •Local health, water and sanitation plan; •Local food resilience plan; •Development permits. |
•Census of local symbiotic urban activities (urban symbiosis, industrial symbiosis, ecological symbiosis), Profiles of local urban metabolism; •GIS of urban land for resilience logistics; •GIS of green land and agricultural capacities. |
||
|
Education, teaching and research |
•Popularisation and local scientific information; •Masters in major risks, thematic urban projects (health, intelligent transport, green urban development); •Continuing professional education for architects, town planners and developers in major risks and urban resilience; •Research projects on flexible planning and construction techniques and technologies, toxic waste treatment, HSE management, expertise and assessment of health vulnerability. |
||||
|
Citizen participation |
•Involvement of local associations, local students, building managers, local start-ups, volunteer professionals, and retired people; •Creation of local contracts for health maintenance, hygiene, and training for young people; •Creation of local agricultural production contracts. |
•Setting up personal assistance agencies (home help, home care, automated transport, robotic delivery, etc.) with the redevelopment of public spaces; •Creation of green networks and corridors, allotments, local urban agriculture plots and farms, and craft workshops. Flexible spaces for co-working, co-production, co-management, etc. |
•Involvement of neighbourhood associations in decisions on total or partial local quarantine (housing estates, neighbourhoods); •Assessment of the social acceptability of health measures (surveys, interviews, expert opinions); •Assessment of the acceptability of the major risk threshold for disaster declaration (decree) and special insurance procedures. |
||
3.2.3 Urban health planning framework for Algiers
At this stage of the study, we can identify the key elements crucial for developing an Urban Health Planning Framework for Algiers. These elements will guide the formulation of strategies tailored to the city’s specific needs and challenges:
The tactical factor "Protection against major hazards" exhibits a consensus around a negative peak for the variable "Evacuation." This necessitates enhancement of technical means and information technologies for warning systems, along with the development of a risk-aware culture through education and training. It is vital to assess the social acceptability threshold of risks and to integrate spaces facilitating accessibility for rescue services and social regeneration into urban planning. Establishing protection perimeters, evacuation routes, and buffer zones for hot spots is also imperative.
Regarding all three factors, local investment by Algiers municipalities in the coming years should be directed towards urban development priorities deemed essential: (i) databases and digitization - (ii) separate technical networks and logistical equipment (water, sanitation, fire-fighting) and decentralised electricity networks - (iii) urban agriculture and local circular economy networks - (iv) high-security sanitary equipment and emergency accessibility logistics equipment (modular road systems, emergency parking for drones and authorised vehicles, heliport, equipped evacuation platforms) - (v) storage equipment (water, mobile generators, medical equipment, hygiene and maintenance supplies, basic foodstuffs, municipal public works fleet) - (vi) local green networks - and (vii) multi-purpose integrated buildings.
Table 6. Urban policy areas identified in Algiers
| Algiers Province Facing COVID-19 | |||||||||||||
| Summary of Local Identified Vital Needs - Exogenous Health Vulnerability Factors (SNAT2030, RRC2035, PNC2030, PDAU2035) | |||||||||||||
| Ecological Crisis | Climate Crisis | Socio-Ecological Crisis | |||||||||||
| - Biodiversity loss | - Microclimate disruption and social risks | - social inequalities | |||||||||||
| - Hydric stress | - Drought and food insecurity | - Unemployment | |||||||||||
| - Depletion of fossil energy resources | - Floods and technological risks | - inadequacy of training | |||||||||||
| - Pollution (soil, air, water) | - Heat stress and health risks | - Poverty | |||||||||||
| - Increase in natural disasters | - Rising carbon emissions and economic risks | - Insecurity and delinquency | |||||||||||
| Urban governance crisis | |||||||||||||
| (city policy, land management and urban finance, urban planning, urban planning, urban programming, local development monitoring) | |||||||||||||
| 1- Operating Autonomy | 2- Proximity to Vital Activities | 3- Risk Protection | |||||||||||
| Endogenous factors of vulnerability and areas of action identified | |||||||||||||
| 1.1 | 1.2 | 1.3 | 1.4 | 2.1 | 2.2 | 2.3 | 2.4 | 3.1 | 3.2 | 3.3 | 3.4 | ||
| Functional adaptation | Functional decentralization | Cross-sectoral innovation and citizen participation | Availability of local resources | Exposure to health risks | Capacity in local equipment and services | Spatial accessibility | Mobility | Securing | Evacuation | Sanitary isolation | Risk management | ||
| engineering infrastructure, Streets and public areas | Information and local communication | Strategic cross-sector urban planning | Land intended for development | Densities and functional composition | Health services: health, pharmacies, civil defence | Urban compactness | Specialized and innovative means of transport | Storage logistics equipment | Emergency routes and evacuation systems | Special reception sanitary facilities | Databases and information | ||
| Multi-purpose building (housing, offices, facilities) | Local production (agricultural, craft, SMEs and SMIs | Urban programming at boundary states | Natural resources: water, energy, food, biodiversity | Emergency Accommodation Capacity | Basic services (food, hygiene, transport) | Temporary parking and waste collection | Organization of short circuits | Mobile emergency equipment | Relay and evacuation platform | Separative network decentralized networks | Urban planning and warning tools | ||
| Green spaces (networks and greening) | Use of local resources | Adapted urban design | Human capital | Environment quality | Urban services (post, telecom, schools, energy, water) | Recreational and sports green spaces | Ability in sports and recreation | Hygiene services | Evacuation areas | Reserves of vital resources | Aid to the population | ||
| Management by objective and projects | Intercommunity and project contract | Participatory local management | local financial resources | Local databases (municipalities health profiles) | Administrative services: municipalities | Sanitary zoning | Accessibility to domestic and outdoor transport | Monitoring service | Emergency shelters | Communications and public information | emergency management | ||
About the operational factor "Proximity of vital activities," as discussed above (point 3.2), there is a lack of consensus. Nevertheless, it is crucial to emphasise that experts' opinions converge on the identified failures related to the variables "Facilities and services" (such as broadband internet, post office, banks, administrations, billing services, and access to nature) and "Availability of urban resources" (including non-strategic and non-participatory planning, programming without considering carrying capacity, inadequate land use, and insufficient local employment opportunities). These failures intensify inequalities between municipalities and are considered alarming, highlighting the need for a thorough examination of the territories, employing modern planning tools like PBO (Planning by Objectives).
Unfortunately, decision makers continue to ignore the necessity of these steps, which are essential to keeping operational urban planning methods. The SEPO analysis revealed this alarming condition. Investing in databases, ensuring equitable access to public housing, services and facilities, and engaging disadvantaged communities as partners in health resilience and territorial and social cohesion are, also recommended for African cities in general [13].
The strategic factor "Local Autonomy of operation" poses the most significant challenge. The majority of experts expressed concern about the municipalities’ lack of autonomy in taking action, considering it a factor that will increase urban vulnerability in the future. The SEPO prospective analysis shows an imbalance between results (barriers to be removed) and hopes (existing requirements and potential), whose balancing is part a strategic approach that requires time.
This study highlights the urgency of acting to strengthening resilience against crises. It recommends, in particular, reviewing the legal texts to integrate health risk, to complement the tools of urban planning with a sanitary dimension, to set up an alert system to monitor the use of resources, to restructure local authorities and to promote local management through projects. By promoting cross-sectoral dialog and citizen participation, these measures will improve the management of vital resources and strengthen the resilience of territories. Table 6 above presents the areas of public policy related to investment considered essential in Algiers. These investments collectively address the imperatives of climate change, adaptation and resilience against significant urban hazards. Their long-term social, economic, and ecological viability is assured. Today’s viral crisis offers an opportunity to prevent the next pandemic from becoming a life-saving crisis for the city and its inhabitants through proactive actions within the scope of urban planning.
A COVID-19 vulnerability assessment based on the full suite of analytical methods (MAG, MCDA, and SFPO) highlights the feasibility of developing an urban health planning framework for Algiers. The main findings are summarized as follows:
The importance of changing the current paradigm of urban planning from the classic ecosystem concept adopted by the sustainable development approach to an organic concept of the city that is now treated as a living organism. The model of health resilience that we propose, based on the extension of the ecosystem sustainability model, goes further in the direction of resilience by considering the city as a living body where each individual, territory, and action, meets the vital needs of the entire organization. The convergence of sustainable cities’ main characteristics has thus highlighted three factors of health vulnerability that are at the foundation of the aspirations of living beings: autonomy of functioning (A), the necessary proximity of action for survival (P), and protection against major hazards (P).
Urgent revision of current approaches, tools and procedures in urban planning in Algeria and elsewhere. The APP factors (Autonomy/ Proximity/ Protection) can be recognized as the main vectors of resilient urbanism, as demonstrated by our reflection. However, it is a question of rethinking the whole foundation of urbanism, moving towards the sense of resilience understood no longer as resistance or the ability to recover from a crisis or disaster, but as a process. The APP process is composed of Autonomy of functioning before the crisis, Proximity to action required for survival during the crisis and protection against other major risks after the crisis.
This study confirmed that in Algiers, the needs of life must be addressed urgently in two stages: short and medium term. The Algiers urban development strategy would be compromised, and the objectives of PDAU 2035 could not likely be achieved. The Urban Resilience Master Plan, currently being developed, could provide a kick-start for the new urban planning approach.
Among the 12 variables analysed by RTSA, five of them strongly contribute to the urban vulnerability of Algiers (Decentralisation, Consultation, Management of Vital Resources, Security, and Evacuation). Conversely, the remaining four variables exhibit rather optimistic results (Equipment and services, urban resources, isolation, and urban risk management).
This research has allowed us to confirm that the therapeutic approach of resilient health planning should be applied to all 57 municipalities in Algiers simultaneously, with degrees of intensity weighted according to local needs and obstacles to be overcome by areas of public action. The results of the SFPO analysis generate a series of findings/recommendations that highlight the parallels between the challenges of climate change (adaptation, mitigation) and the challenges of a global health crisis.
Furthermore, the analysis of local adaptation factors (autonomy, proximity, protection) that concern the five (5) areas of action in urban planning (diagnosis, strategy, programming and planning, development design, and monitoring and management), aligns with the areas of the organic model of urban resilience adopted. This allows the identification of shortcomings and designates the parameters on which action should be taken.
This research has allowed us to confirm that the organic therapeutic approach of resilient health planning should be applied to all 57 municipalities in Algiers simultaneously, with degrees of intensity weighted according to local needs and obstacles to be overcome by areas of public action. Only with joint effort and solidarity could Algiers regain its strength in the face of future threats.
Only with joint effort and solidarity could Algiers regain its strength in the face of future threats. Therefore, this study opens the way for more in-depth and closer to the territory analyses. We encourage future research to continue developing this topic by recognizing that biological threats during a pandemic are likely to recur in the future and cumulate their adverse effects with other major risks.
Appendix A. Extract from the RTSA grid under SFPO analysis
|
|
1.2 DECENTRALIZATION |
1 |
2 |
3 |
4 |
5 |
|
|
a) |
Local public communication networks within the municipality do not exist, information on projects and investments is centralized and controlled, and the initiative towards autonomy of local public action is hampered. |
x |
x |
x x x x |
x x |
|
Citizen participation in decision-making is not effective, the experience of Co-Ville workshops has not been developed. Local initiatives exist, develop in the municipalities and propose practical solutions according to the needs identified, but encounter logistical difficulties. |
|
b) |
Local production, in the secondary and tertiary sectors, is oriented towards making the municipality attractive (PDAU 2016), not towards meeting local needs; local productive or competent human resources are not inventoried; Financial resources are centralized and distributed top-down. |
x x |
x |
x x x x x |
|
|
Several local production and service initiatives with the help of digital technologies (applications, associations, social networks, and workshops) are operational in some areas but suffer from regulatory and financial constraints. |
|
c) |
Local resources (land; natural: water, energy, forests, agricultural lands; human: professional skills, associative; financial from local taxes; logistics and technology) are managed centrally, do not benefit the municipality and do not target the control of major urban risks. |
x x x x x |
x x x |
|
|
|
Current policy trends in energy transition and urban resilience open the prospect for decentralization of certain areas of local management (integrated management of urban and special waste, industrial symbioses, solar energy installations, and urban agriculture), decentralization of technical infrastructures and logistic equipment. |
|
d) |
The urban covalence of neighbouring communal entities holding resources to be exchanged or shared is not possible at present, due to the centralization of local budgets and territorial management dependent on central provincial authorities. |
x x x x |
x x |
|
x x |
|
Law 06-06, the 2018 finance law, the PDAU of Algiers 2016, introduce the notion of shared and participatory local development, subject to the partnership contracting of local development projects, but it is not supported by the regulations. |
|
e) |
Number of opinions expressed by situation |
12 |
7 |
9 |
4 |
0 |
|
Situations related to: Information & Communication/Local production/Use of local resources/Intercommunity
|
|
Retrospective (Successes / Failures) |
Prospective (Potentials / Obstacles) |
|
positive |
|
|
|
Negative |
|
|
|
3.2 EVACUATION |
1 |
2 |
3 |
4 |
5 |
|
|
|
e) |
The medical evacuation of infected persons in a pandemic situation is carried out by using the existing road network to hotels identified as emergencies and sometimes converted. No other route of evacuation is planned. |
x x x x |
x x x
|
|
x |
|
Specific equipment (P4 laboratories and safe reception centres) requires a location outside the urban fabric and an adapted layout (safe accessibility). Drones, helicopters and jets need the spaces identified in the urban fabric, but the urban programming does not provide for any allocation in this direction. |
|
f) |
The protection of people against the effects of disasters (injured, intoxicated, sick, elderly, disabled, and children) is not envisaged as an urgent action to develop public spaces in Algiers. |
x x x xx |
x |
x |
x |
|
Areas reserved for victims are not indicated in the urban development plans (assembly sites, equipped relay platforms, evacuation circuits, heliports, storage centres for sanitary equipment, water, renewable energy plants, basic power) |
|
g) |
Evacuation of the population in case of an imminent danger (fires, tsunami, explosion) |
xx xx xx |
x |
|
|
x |
PRPs and Disaster Behaviour Guides are not disseminated to civil society, nor accessible on specialized professional platforms |
|
h) |
Disposal of hazardous or toxic waste is only covered for organic or chemical waste from the care units, radioactive waste, electronic waste, electrical waste, etc. are not separately collected or treated. |
x |
x |
x |
x x x |
x x |
The development of public spaces does not include specific waste collection, sorting and treatment sites. Urban planning is flawed, with units of this type requiring specific land and protection. |
|
|
Number of opinions expressed by situation |
16 |
6 |
2 |
5 |
3 |
|
Situations related to: Evacuation sanitaire/Evacuation de protection/Evacuation de sureté/Assainissement
|
|
Retrospective (Successes / Failures) |
Prospective (Potentials / Obstacles) |
|
positive |
|
|
|
Negative |
|
|
[1] Lévy A. (2012). Ville Urbanisme et Santé, les Trois Revolutions. Mutualité Française: Pascal.
[2] S2D, International Association for the Promotion of Health and Sustainable Development. (2000). The Healthy-Cities movement, Urban action for health and sustainable development, City of Rennes, European Centre for Urban Health, Copenhag.
[3] MATE. (2004). Law no. 04-20 of 25 December 2004, on the prevention of major risks and disaster management in the context of sustainable development. Ministry for Spatial Planning, the Environment and Urban Affairs, Algiers. https://www.joradp.dz/HAR/Index.htm.
[4] GPN (Global Planners Network). (2020). Declaration of World Town Planning Day. https://www.cip-icu.ca/.
[5] UNESCO (United Nations Educational, Scientific and Cultural Organization). (2020). Journée Mondiale de la Ville, Rapport final, Paris. https://www.unesco.org/fr/sustainable-cities/world-cities-day-2020.
[6] WUF (World Urban Forum). (2020). New Urban Agenda 2030, 9e Forum Mondial de l’Urbanisme, Kuala Lumpur. http://www.wuf9.org/.
[7] Hossain, Z.A.N.M. (2021). Sustainable development and livelihoods of Rohingya refugees in Bangladesh: The effects of COVID-19. International Journal of Sustainable Development and Planning, 16(6): 1141-1152. https://doi.org/10.18280/ijsdp.160615
[8] Wilkinson A. (2020). Local response in health emergencies: Key considerations for addressing the COVID-19 pandemic in informal urban settlements, Environment and Urbanization, 32(2): 503-522 https://doi.org/10.1177/0956247820922843
[9] Dutta, A., Fischer, H. (2021). The local governance of COVID-19: Disease prevention and social security in rural India. World Development, 138: 105234. https://doi.org/10.1016/j.worlddev.2020
[10] Daoudi-Tamoud, M. (2022). Urban health performance assessment tool for an urban public health project in Algiers. PhD thesis, EPAU, Algiers.
[11] Boughedir, S. (2015). Case study: Disaster risk management and climate change adaptation in Greater Algiers: Overview on a study assessing urban vulnerabilities to disaster risk and proposing measures for adaptation. Current Opinion in Environmental Sustainability, 13: 103-108. https://doi.org/10.1016/j.cosust.2015.03.001
[12] Barbera, C., Jones, M., Korac, S., Saliterer, I., Steccolini, I. (2021). Local government strategies in the face of shocks and crises: The role of anticipatory capacities and financial vulnerability. International Review of Administrative Sciences, 87(1): 154-170. https://doi.org/10.1177/0020852319842661
[13] UN Habitat. (2020). Impacts of the pandemic in urban areas, secretary-general’s policy brief on COVID-19 in an urban world. https://unhabitat.org/sites/default/files/2020/07/final_q_and_as_for_un_secretary-generals_policy_brief_on_c19_in_an_urban_world_2.pdf.
[14] Sidi Boumedienne, R., Guerroudj, T. (2013). Echec des Instruments ou Instruments de l’échec? Alternatives Urbaines, Alger.
[15] ONS (Office National des Statistiques). (2019). https://www.ons.dz/.
[16] MHUV. (2016). Master Plan for Urban Planning and Development in the Wilaya of Algiers, DE n°16-319 of 5 December 2016 approving the PDAU of Algiers. Ministry of Housing, Town Planning and Urban Affairs, Algiers. https://www.joradp.dz/HAR/Index.htm.
[17] Hocine, M. (2021). Proposing SMaR²T-ATi, an assessment tool for urban sustainable development and experimentation on Eucalyptus municipal territory, Algiers province. Land Use Policy, 101: 105177. https://doi.org/10.1016/j.landusepol.2020.105177
[18] Alsalem, M.A., Alamoodi, A.H., Albahri, O.S., et al. (2022). Multi-criteria decision-making for coronavirus disease 2019 applications: A theoretical analysis review. Artificial Intelligence Review, 55(6): 4979-5062. https://doi.org/10.1007/s10462-021-10124-x
[19] Malakar, S. (2022). Geospatial modelling of COVID-19 vulnerability using an integrated fuzzy MCDM approach: A case study of West Bengal, India. Modeling Earth Systems and Environment, 8(3): 3103-3116. https://doi.org/10.1007/s40808-021-01287-1
[20] Froidevaux, D. (2007). Project approaches, Public Health Action Seminar PHA, Genève, 15 p.
[21] Daoudi-Tamoud, M. (2022). Integrated “SaMU” method for assessing health performance in cities for an urban public health project in Algiers. Algerian Journal of Environmental Science and Technology, 8(3): 2654-2666.
[22] Beier, M. (1994). Participatory evaluation using the SFPO method. https://pace-consultants.de/exemples/sepo_ma_e.pdf.
[23] Lincoln Institut of Land Policy. (2019). Resilient Communities Program. http://www.lincolninst.edu/.
[24] Berezowska-Azzag, E., Abdelatif, I., Akrour, N., Azoui, O., Srir, M. (2015). Baromètre des performances urbaines locales, Alger et ses communes (Barometer of local urban performance, Algiers and its municipalities): Green city index; Actif city index; Lively city index. Alger. Editions Alternatives Urbaines: 174.
[25] Berezowska-Azzag, E. (2012). Projet urbain, guide méthodologique. In Comprendre la déMarche du Projet Urbain. Synergie, Algiers.
[26] Daoudi-Tamoud, M., Berezowska-Azzag, E. (2021). La verdure comme remède aux pathologies urbaines. Compensation des nuisances urbaines par la verdure, au service d’évaluation des performances sanitaires locales. Algerian Journal of Environmental Science and Technology, 7(2): 1897-1909.
[27] Sarkar, C., Webster, C. (2017). Urban environments and human health: Current trends and future directions. Current Opinion in Environmental Sustainability, 25: 33-44. https://doi.org/10.1016/j.cosust.2017.06.001
[28] de Leeuw, E., Simos, J., Forbat, J. (2020). Urban health and healthy cities today. In Oxford Research Encyclopedia of Global Public Health. Oxford, UK: Oxford University Press.
[29] Gatzweiler, F., Fu, B., Rozenblat, C., et al. (2021). COVID-19 reveals the systemic nature of urban health globally. Cities & Health, 5(sup1): S32-S36. https://doi.org/10.1080/23748834.2020.1763761