Haitham Alsabi![]() | Mohd Saiful Izwaan Saadon
| Mohd Saiful Izwaan Saadon![]() | Al Montaser Mohammad*
| Al Montaser Mohammad*![]()
© 2023 IIETA. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
The ongoing COVID-19 pandemic in Jordan has brought terrifying effects on hospital management performance worldwide. The ultimate purpose is to generate empirical knowledge and open research opportunities into future studies. Investigating critical resource-based factors would significantly contribute to the growing body of knowledge that informs policies and programs for mitigating the negative effects of the pandemic on the administration of Jordan's healthcare sector. To this end, we surveyed a sample of 418 managers in the Jordanian health sector. To produce numeric data and to test the hypotheses, the researchers employed structural equation modeling, specifically using the PLS-SEM technique. This study argues that the COVID-19 pandemic has had a profound negative impact on hospital performance in Jordan. Telemedicine, innovation, and infrastructure exhibit a significant and positive direct influence on management performance. As a result, this study accepts two hypotheses pertaining to the moderating influence of telemedicine and infrastructure in mitigating the negative consequences of COVID-19 on performance. However, the hypothesis related to the moderating role of innovation in the impact of COVID-19 on performance is rejected. The pandemic has presented unprecedented challenges to the healthcare sector, necessitating the development of effective management strategies to address the surge in patient volume and resource constraints. Telemedicine and healthcare infrastructure have been identified as critical resources with a significant moderating effect on healthcare management performance during this crisis. Telemedicine, as a technology-related resource, enables remote healthcare delivery, virtual consultations, and monitoring, which have become crucial during the pandemic.
COVID-19 crisis, healthcare performance, infrastructure, innovative, Jordan, PLS-SEM, quantitative
The public/semipublic sector and the private sector make up Jordan's healthcare system. Both sectors include hospitals, primary care offices, pharmacies, and other ancillary services. Given the recent population expansion and the significant influx of refugees into Jordan, the current bed rate is judged insufficient. 5 Jordanian primary health care clinics provide immediate access to medical care along with services for chronic illness management, pregnancy and childcare, and vaccines. They operate in both urban and rural settings and range in size from small individual clinics to huge multiclinic complexes, depending on the location and people served. Home healthcare services are few in Jordan and are mostly offered by the private sector. Home care services are intended to reduce treatment costs, but because they are not covered by public or private health insurance, the majority of Jordanians cannot afford them [1].
Patients are required to stay in acute care facilities for lengthy periods of time (up to several months in some situations) since Jordan lacks long-term care facilities. As Jordan's population ages, long-term care facilities and home health care services are required to reduce the burden on acute care resources. In addition to the public and commercial sectors, the United Nations and nonprofit humanitarian organisations contribute a large percentage of Jordan's health care [2].
The United Nations Relief and Works Agency (UNRWA) offers beds or pays a portion of the cost of inpatient care at public and private medical facilities to help refugees who need hospital treatment. The Jordanian Ministry of Health has been assisting the UN High Commissioner for Refugees (UNHCR) in providing medical care to Syrian refugees in camps for the past few years. On the other hand, the needs of the larger population of refugees living outside of the camps are not adequately met. Up to the end of 2014, the Jordanian Ministry of Health provided free medical care to all Syrian refugees who had registered with the UNHCR [3].
Free health care access was abolished, nevertheless, as a result of the huge financial burden this placed on the healthcare system. As a result, Jordanians without insurance and Syrian refugees living outside of the camps both have to pay the same out-of-pocket expenses. Even though fees at public institutions are frequently waived, many poor families may still find it extremely difficult to cover this cost. Due to the cost, such families may decide against receiving medical care, especially for chronic conditions that don't require immediate attention. There is no national electronic health records system in Jordan, and each sector of the healthcare industry operates independently [4].
Jordanian healthcare facilities were badly impacted by the COVID-19 issue and faced numerous difficulties and pressures because of a lack of resources to contain the situation [5]. Notably, frontline workers in the healthcare industry were at a significant risk for developing mental health conditions such as stress, sleeplessness, despair, and anxiety [6]. The additional workload, and managing a large number of patients, with little access to the resources also caused health staff to feel frustrated and hopeless [7]. These all factors eventually caused a severe crisis in the performance of healthcare centers. Literature has overlooked the role of these factors in the impact assessment of crisis situation and healthcare management performance. This study, therefore, aims to bridge this literature gap and examines ways in which the healthcare management has been hampered and also come up with factors that could help healthcare sector to overcome the daunting effects of the COVID-19 pandemic and other similar potential situations.
2.1 COVID-19 and the healthcare management performance
10.6 million people live in Jordan, a nation in the Eastern Mediterranean, which has an area of 89,342 square kilometres. [8-10]. Jordan shares borders with Saudi Arabia, Syria, the occupied Palestinian territories, and Iraq. With a GNI per capita of 9,430 USD in 2018, the World Bank has reclassified Jordan as an upper middle-income nation [11, 12]. Since the start of the COVID-19 pandemic, the Jordanian government has adhered to the recommendations and updates from the WHO [13].
Several preventative and control measures have been developed at the local and national levels to restrict the spread of COVID-19 inside Jordan. Through a coordinated multidisciplinary team at the National Centre for Security and Crises Management (NCSCM), the government of Jordan is taking the lead in the fight against COVID-19. The crisis task group will collaborate to identify and carry out the best evidence-based recommendations feasible. It is made up of specialists from several ministries, industries, and organisations. Official authorities carefully and continually update and communicate information to the public about various life views [14].
Additionally, teams of experts in epidemiological surveillance are at work around the nation to resolve incidents and provide random viral testing and surveillance. In addition, the government releases daily updates to the public detailing the number of confirmed cases, recoveries, and fatalities. The Ministry of Health and the Ministry of Digital Economy and Entrepreneurship worked together to create the COVID-19 website in Arabic, which aims to enlighten the public about the most recent advancements in digital health [15].
Jordan is a well-liked travel destination and a key hub for many regional flights and journeys; as a result, and in light of the growing number of COVID-19 cases globally, the government has started to implement (periodically revised) strict rules and measures in the areas of travel, education, religious and social events, as well as employment in various industries. The initial step in preventing and controlling the spread of COVID-19 in Jordan was to undertake temperature tests of incoming visitors and place those who arrived from nations where COVID-19 was common under a quarantine. To reduce the spread of COVID-19 in Jordan, the national defence law was declared on March 17, 2020, which represented a turning point in the nation's prevention and control efforts [16].
According to this research, significant levels of discomfort may also be caused by prejudice, contempt, stigma, and a lack of moral support for healthcare staff. Gerada and Jones [17] found that among healthcare professionals, surgeons are the least likely to ask for help. Help for mental health difficulties despite the signs they show, such as sadness and exhaustion. Their reluctance is strongly correlated with worries about losing their professional credibility as physicians and the stigma associated with poor performance, so they must seek assistance from the medical community. Elevated levels of PTSD and sadness were seen in COVID-19 [18]. Some nations, notably the United Kingdom, have created counseling programs to aid healthcare professionals in coping with persistent pandemic-related stress due to the negative consequences of acute and chronic psychological anguish. According to Wang et al. [19], when workers experience chronic working stress that is adequately managed, stress, burnout syndrome, which is defined by the International Classification of Diseases 11th Revision as an occupational phenomenon, arises. The difficulties that healthcare personnel experienced both personally and professionally during the personal stressors have a knock-on effect on performance at work, which strains the healthcare system and eventually has an impact on population-level illness outcomes. This is the first wave of COVID-19 [20]. Despite knowledge that COVID-19 had a negative impact on healthcare workers' mental health and research highlighting the importance of providing ongoing, accessible mental healthcare for healthcare workers, few healthcare workers sought out mental health support [19-21]. Dykes During the implementation of public health programmes at a societal level, healthcare employees may feel greater stress as a result of their already demanding workloads, workplace adjustments, and caregiving obligations, which has a negative impact on management performance.
Based on above discussion following hypothesis can be proposed.
H1: COVID-19 negatively impacts healthcare management performance.
2.2 Effects of telemedicine, innovation, and infrastructure on the healthcare management performance
Tahan [22] provided significant case management approaches and solutions in response to the recent coronavirus disease (COVID-19). The show highlights the importance of skilled case managers in managing crises like a pandemic over the world. The revised tasks and obligations of case managers and their leaders in addressing the needs of patients and support systems during the crisis are further described in Part II. It focuses on the growth in end-of-life care requirements, their effects on case management for workers' compensation cases, and the obligations placed on professional case managers in terms of self-care. suitable for usage throughout the health and human service continuum in a range of case management practice situations, with an emphasis on acute care.
Xiao et al. [23] evaluated the effects of the SARS-CoV-2 pandemic on the use of health services in China using data from the normal health information system collected over a period of almost four years. They conducted a retrospective observational cohort analysis of health care utilisation from all tiers of mainland Chinese healthcare institutions. They looked examined monthly all-cause health facility visits and the number of inpatients in medical facilities before and throughout the SARS-CoV-2 pandemic using data from the national routine health information system from January 2016 to June 2020. They used segmented negative binomial regression and interrupted time series analysis to examine changes in healthcare utilisation brought on by the epidemic.
An area-level measure of socioeconomic position known as the Human Development Index (HDI) was used to stratify studies by facility type and province in order to look at potential variations in impacts. Prior to the SARS-CoV-2 pandemic, a positive secular trend in healthcare consumption habits was seen. During the SARS-CoV-2 outbreak, we observed statistically significant reductions in all indices, with each indicator's low point occurring in February 2020.
In high HDI regions, all-cause hospital visits decreased by 63 percent (95 percent CI 61-65 percent; p0•0001), while all-cause visits to primary care clinics decreased by 71 percent (95 percent CI 70-72 percent; p0•0001), while inpatient volume decreased by 33 percent (95 percent CI 24-42 percent; p0•0001), and outpatient visits decreased by 10% (95 percent CI 3-17 percent). More outpatients were discharged than there were visits to the medical facility (51 percent versus 48 percent; p 0•0079). Hospitals had higher declines in both inpatient volume and visits to health facilities than did primary care facilities (p0•0001), and developed regions experienced greater declines than underdeveloped regions.
Due to altered patient and provider behaviour, the closure of medical facilities or non-emergency services, severe mobility restrictions, and perhaps a lower risk of non-SARS-CoV-2 diseases, China's use of inpatient and outpatient health services decreased dramatically after the SARS-CoV-2 outbreak. All indicators started to get better in March, but most still hadn't returned to their pre-SARS-COV-2 levels by June 2020.
The present coronavirus illness (COVID-19) crisis, Ghanemi et al. [24] has compelled governments to put in place measures including mask use, physical isolation, increased cleanliness and disinfection, as well as house confinement and economic closure. Such policies have gravely detrimental effects on the economy and public health. However, given that they contribute to improving some aspects of population health, these same policies also have positive "side effects" that are worthwhile mentioning. Wearing a mask, for example, can assist to minimize allergies and the spread of other disease-causing germs in the air.
Physical separation and limiting social interaction assist to prevent the transmission of infectious illnesses, while economic closure can help to lessen pollution and the health issues that come with it. These favorable "side effects" may encourage decision-makers to address and prevent illnesses such as allergies, infectious diseases, and noncommunicable diseases, as well as enhance health care and pathology management. Indeed, the efficacy of such measures in addressing specific health issues inspires COVID-19 measures to be used in the management of specific health issues. With the huge harm COVID-19-related measures have made to nations' economy and people's lives, health care experts and decision-makers must discuss how to balance the benefits and drawbacks of these policies to further optimize them.
The provision of healthcare to patients who are unable to leave their homes is one of the challenges that Kronenfeld and Penedo (2021) showed the novel Coronavirus (COVID-19) produced by the SARS-CoV-2 virus has caused around the world. Although health care doctors have long utilised telemedicine—the use of electronic information and communications technology to assist and promote long-distance clinical health care—it wasn't until the COVID-19 pandemic that it became extensively used. It has now evolved into the main means of patient treatment during the COVID-19 outbreak. Patient access is the most hardest obstacle to overcome, even if hospitals and providers also have difficulties in creating these services. Patients need advanced technology support, translation services, and other safeguards in order to feel secure engaging in a telemedicine conversation.
In addition, proper follow-up for chronic medical disorders and malignancies must be provided, assisting in the prevention of these problems worsening during the COVID-19 crisis. Finally, we must guarantee that all patients seeking health care, especially those with lower socioeconomic standing, are treated equally. Several of these patients use the internet through public hotspots or library computers, which is unlikely to be conducive to a therapeutic meeting. To promote health equity for all patients seeking care, these barriers must be removed. During this moment of crisis, telemedicine may link patients and clinicians, and it may serve as a model for future usage once the epidemic has passed.
Zhong et al. [25] examined the potential connection between the usage of telemedicine and the toll that the coronavirus took on mental health at the height of the COVID-19 pandemic in Wuhan. Based on the Crisis and Emergency Risk Communication Model and the Health Belief Model, it presents a conceptual model to investigate how people in Wuhan—the initial epicentre of the global COVID-19 epidemic—used innovation on social media and its effects on users' mental health states and health behaviour modification. Their research found a connection between the invention of social media usage and melancholy and secondary trauma, as well as a connection between changing health behaviour and using telemedicine. However, no connection between alterations in health behaviour and concerns with mental health was discovered. Residents of Wuhan discovered that exchanging health information via the invention of social media gave them knowledge, emotional support, and peer support when the virus struck. On the other side, excessive telemedicine use, social media innovation, and infrastructural improvements have improved mental health. Their research revealed that utilising telemedicine to take innovation of social media breaks during the pandemic would enhance wellbeing, which is crucial for minimising the impact the epidemic does to mental health.
H2a: Telemedicine positively affects healthcare management performance.
H2b: Innovation positively affects healthcare management performance.
H2c: Infrastructure positively affects healthcare management performance.
2.3 Telemedicine in the effect of the COVID-19 Pandemic on healthcare management performance
Organizations have acknowledged that telemedicine is playing a vital function during the COVID-19 pandemic, establishing their divisions to promote telemedicine [26]. Present and emerging telecommunications systems play a vital role in exchanging valid knowledge for illness and accident diagnosis and treatment. Telephone consultations, automated fracture clinics and video consultations are the major modalities for remote consultations now [27]. Such developments will be a central element in how we provide health services in the future.
Telecommunications Systems: Because of COVID 19, telemedicine or the provision of health care facilities using communication or information technologies has recently advanced throughout the world. In a post-Covid-19 world, telemedicine is poised to change healthcare. Governments around the world have introduced tele-consultation programs, which are compulsory for providers of health care. Via this service, patients may seek medical advice by video and audio. This program would also allow people living in the most remote areas to obtain health-related consultations [28]. Recently, the medical association has introduced the requisite legislative mechanisms to encourage the universal use of telemedicine and, in a few cases, has provided recommendations on its use. Doctors would tend to treat patients immediately after the pandemic stops, but at the same time, thanks to improved telemedicine expertise, they would help them treat patients if they miss clinic appointments.
Training and Education: Of all specialties, teaching is a compulsory component of medical training. To continue providing training sessions to trainees at variable stages, numerous online tools have been used. This has proved to be more realistic, versatile, and instructional. Conferences, workshops, seminars, and other types of remote training are made possible by mobile technologies [29]. Hospital rounds were filmed by webcams; Zoom classrooms, interactive simulators, 3D images replaced cadavers, webcasting, video chat rooms, interactive dissection, interactive virtual reality E-anatomy have now been taking place [30].
Patient Perception and Factors: Traditionally, orthopedic surgeons issued referrals prior to the pandemic and had to consult patients on certain symptoms (such as swelling of the ganglion etc.) [29]. Patients with these problems were advised over the telephone during the pandemic and directed to online services that satisfied them. It is believed that the knowledge and encouraging message that can be given through visiting specified online websites and online physiotherapy facilities will help patients with certain conditions. It saves a lot of appointment time and manages to unload the outpatient clinics and health care facilities.
Telemedicine is "the use of medical information exchanged from one site to another via electronic communications to improve a patient's health status," according to the American Telemedicine Association [31]. The term can be used to describe a variety of health-related services thanks to the broad scope of this definition. These services include telephone interactions, electronic transmission of clinical data, electronic messaging services, electronic alerts, and many others [32]. The breadth of the parties participating in this information exchange is expanded if this wide definition is taken to mean that it can happen not just between healthcare providers and patients or their carers but also between various healthcare providers. There are telemedicine services available in many different health professions [33]. Different environments might have quite different telemedicine delivery objectives and strategies. In the present, Moore and Woodcock [34], found that prescribers (physicians and physician extenders) contact with patients through telemedicine more frequently during acute illnesses or when other obstacles to care make in-person consultations difficult. It is also commonly utilised to establish connections between healthcare team members and clinical professionals to offer consultations in circumstances when specialised services might not be accessible [35].
The need for healthcare has become universally recognised as a basic human necessity. This is perhaps one of the most important assertions, regardless of where in the globe you live: developed, developing, or undeveloped. Unfortunately, many nations are unable to provide their citizens with enough high-quality healthcare services owing to a lack of infrastructure and skilled medical personnel. E-health was considered as a way to prevent or reduce inequities. E-health, as defined by Lepore [36], is the term used to describe planned health services supplied online. This involves giving access to healthcare professionals and providers via a variety of technologies, such as computers, mobile phones, websites, and applications [37]. Recording and storing administrative and medical data about patients is required to increase the efficacy of doctors' professional actions [38]. To improve patient care quality and health outcomes, to reduce health costs, and to increase the efficiency of doctors' professional activities [39]. Information and communication technology (ICT) is used in the field of e-health to combine various concepts: (1) Without the requirement for user input, sensors are used in telecare to identify particular dangers or collect data; (2) specialised medical equipment is used at home in telehealth to monitor patient health by scanning for possible problems or taking physiological measurements. Telehealth combines linked devices and cloud computing to improve patient-centered treatment and save expenses [40]; (3) Telemedicine, also known as teleconsultation [41], employs interactive audio-visual and data communications to reduce waiting times and medical costs [39], improves patient care and staff productivity [42], and eliminates inconveniences associated with hospital visits. Telemedicine is a helpful technique for preventing hospitalisation for the elderly or those with certain ailments, such as diabetes or cardiovascular issues. Modern technology shouldn't, however, be used to further marginalise people and exacerbate the digital divide [43].
By examining the factors that influence patient behavior toward the adoption of telemedicine health services, the current research thus fills the research gap. During the COVID-19 crisis, both patients and doctors have benefited from telemedicine health services [44]. Because COVID-19 is both fatal and contagious, precautionary measures like human distance can save a patient's life. In the COVID-19 pandemic crisis, it has been observed that healthy people become affected when they visit hospitals. Telemedicine health services are therefore required as an alternative method of health care delivery. In Africa, a health system based on telemedicine applications has been found to be effective in providing, reporting, and tracking patient health care services for Ebola and malaria [45]. Management performance is a subjective assessment that telemedicine can improve the user's health quality [46]. The study will also find that the most important factor in determining the adoption of medical technology is to improve management performance.
Based on the above discussion the following hypothesis can be proposed.
H3: Telemedicine moderates the relationship between the COVID-19 pandemic and healthcare management performance.
2.4 Innovation in the effect of the COVID-19 Pandemic on the healthcare management performance
The Oxford government response tracker for COVID-19 recognized nine elements relevant to lockdowns, which survey the general severity of the actions [47]. These include general travel restrictions, workplace closures, gathering restrictions, postponements of public events, suspensions of public transit, and closures of schools and workplaces. The majority of nations provide individuals with access to necessities like pharmacies and grocery shops, but there are sometimes stringent regulations like maintaining a certain social distance and restricting the number of people who may enter a business at once. Increased stringency is directly linked to a decrease in individuals' overall mobility. For example, Hussain et al. [48] found that a country's fruitful execution of friendly removal has been related to higher rigidity levels in that. In several nations, strict interventions were also linked to changing citizens' behavior to implement social distance [49]. Simulated models and observations of limited country-level data hint to a decrease in overall cases and enhanced pandemic control if tight measures are established and followed [50].
Studies comparing innovation and creativity at the national level are typically contradictory with some arguing that Eastern nations are probably going to score worse on overall originality than Western ones [51]. This is frequently attributed to these nations' cultural makeup and the traditional debate between individualism and collectivism Hofstede's dimensions [52]. According to Morris et al. [53], additional evidence suggests that countries in the Western world place a higher value on usefulness than they do on novelty. This was also observed empirically, with both American and Taiwanese teams exhibiting equal originality in their idea generation.
According to Wang et al. [54], the use of programmed innovations, such as computerized inspection frameworks, may ensure that manufacturing operations continue even during lockdown conditions and can slow the rapid spread of new Coronavirus infections. Adopting an additive manufacturing system, according to Tareq et al. [55], could assist manufacturing companies in meeting the rising demand from consumers in the event of a pandemic. Customers from throughout the globe. Robotic devices and automation systems will be employed in more facets of life than previously imagined, as predicted by Wang et al. [54]. Nambisan et al. [56] observed the industry's ongoing boom in mechanical technology and robotization. Automating chores that the social distancing approach cannot be used for during the COVID-19 epidemic is its main goal. Since the last two decades, mechanization innovations like cloud production and artificial intelligence have become commonplace and brought financial benefits and disruptions to the manufacturing industry and have increased management performance. Their use during a pandemic is now being addressed [54].
H4: Innovation moderates the relationship between the COVID-19 pandemic and healthcare management performance.
2.5 Infrastructure in the effect of the COVID-19 Pandemic on healthcare management performance
Jordan has 106 commercial and public hospitals with a combined bed capacity of 12081. 67 percent of these hospital beds are provided by the public sector, with the remaining portion coming from private organisations. Around 18 beds per 10,000 people are available in hospitals in Jordan, which is more than most other Arab countries in the region but lower than the global average [57].
Health Care Service Capacity was an increase in the capability of mass critical care during this pandemic, suggesting an extension of the capability of intensive care units to handle as many patients as feasible. Personnel, equipment, space, and structure are the four essential elements of surge capabilities. E.g., During the pandemic, numerous hospital units have been raising the ability of ventilators and intensive care beds (e.g., NHS Nightingale hospitals) over the last couple of months. The post-COVID-19 plan to restore elective surgery will help to offer this expanded capacity [58].
Equipment: A backlog and storage/stockpile of ventilators has been installed by the NHS. For the present NHS and possible pandemics, it would be helpful. To generate vast quantities of continuous positive airway pressure (CPAP) units, a team of engineers from the University of London and Formula One engine manufacturer Mercedes have been constantly working. 10,000 devices were shipped within one month to reach the goal of the UK government [59]. This has highlighted the versatility of both community sectors and the spirit of support and cooperation to reach out during a crisis.
The Coronavirus outbreak has compelled nearly every representative of the world to work in something completely different from what they were doing previously. Coronavirus-triggered intercessions such as social separation, travel restrictions, virtual or distant labor, and other groups have compelled the continuation of previous processes, thereby influencing the way in which representatives are on the field [60]. Such interventions to improve the infrastructure triggered by a Coronavirus flareup demonstrated typical behavioral alterations, which can develop with varied lockdowns ranging from brief to long-term. COVID-19's expansion has caused organizations to make efforts to mitigate its influence on employee performance. Most of the focus in activities the board researched up to this point has been directed at determining the impact of Coronavirus flare-ups on associations.
Adopting infrastructure for performance management systems is done with the goal of attaining alignment, a common knowledge of the deliverables, and the methods (such as mentoring, training, and so on) of accomplishing those objectives. Employees' poor performance is driven by a lack of alignment and common knowledge of deliverables when these systems' relevance and validity dwindle. This is especially relevant now, in the aftermath of the COVID-19 epidemic, Hartmann and Lussier [61] explored using a study of practitioner-oriented literature, an interview with workers of organizations, and a webinar with sales professionals. Employees were affected by the pandemic. Using Leavitt's organizational change infrastructure and resource-based view theory, they synthesized a thorough debate on the issues faced by the COVID-19 epidemic, which can impair management performance.
Based on the above discussion the following hypothesis can be proposed.
H5: Infrastructure moderates the relationship between the COVID-19 pandemic and healthcare management performance.
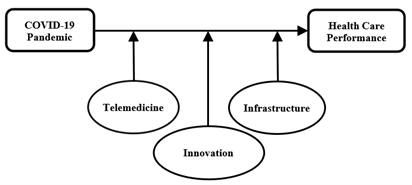
The conceptual model that guides this study is shown in Figure 1.
Figure 1. Conceptual framework
3.1 Sample and data collection
Respondents independently completed self-administered online survey that served as the data collection tool. Because it was simple to use and handle the data, this study used an online questionnaire. Additionally, the respondents were more autonomous and took 5-10 minutes to answer the questionnaire. All respondents were given three weeks to complete the questionnaire before we collected them back. We ensured that all the information from the respondents kept secret and only used for academic purposes. According to Jordanian ministry of Health, approximately 1359 healthcare managers constitute total population of the study, which are selected as the respondents [62]. In choosing the respondents for the current study, consideration was given to their level of familiarity with the subjects of the inquiry. The sample size for this study is 299 managers in the Jordanian health sectors, according to the G*Power (2017) calculator. In order to limit the amount of sampling error and mistakes that may occur during the data collecting process, the sample size was increased by 40% of the original sample size, which is equivalent to 119 questionnaires (299+119=418), in order to obtain more trustworthy and consistent findings.
3.2 Construct measurement
The COVID-19 Fear is a self-reported measure that assesses the fear of COVID-19 pandemic. The scale has seven items that relate to people's emotional responses to the pandemic's fear. These seven items are adapted from the previous studies of Ahorsu et al. [63] and Wang et al. [54]. Innovation is measured as the extent to which organization engages in innovative activities, experiments with new goods or services, and drives new processes. This study incorporates two vital aspects under innovation which are leadership innovation and process improvement. A total of seven items were adopted from Yoon et al. [64] to measure the innovation variable. Infrastructure is measured as the extent to which the hospital has quality infrastructure. It is measured based on three major infrastructure components including basic amenities, infection prevention, and equipment with five items each. Hence, a total of fifteen items were taken from Leslie et al. [65] to measure the infrastructure variable. Telemedicine is measured as the extent to which organization uses telemedicine in their patient care services. This study incorporates the usage and effectiveness of telemedicine in the healthcare organizations. A total of ten items were adopted from Chau and Hu [66] to measure the telemedicine variable. Hospital performance is measured based on the perception of respondents regarding efficiency, staff satisfaction, and patient satisfaction. A total of seven items were adapted from Cleven et al. [67] to measure the hospital performance. A 5-point Likert scale is used to measure the responses, which ranges from 1=strongly disagree to 5=strongly agree. Table 1 shows the constructs of conceptual definitions and the measurements.
Table 1. Constructs definitions measurement
|
Construct |
Conceptual Definitions |
Construct Measurement |
|
COVID-19 Pandemic |
The SARS-CoV-2 virus causes Coronavirus Illness (COVID-19), an infectious disease. |
(Ahorsu et al., 2022) (Wang et al., 2016) |
|
Innovation |
The adoption and implementation of novel practices and processes in the period of pandemic or crisis to enhance management performance. |
(Yoon et al., 2018) |
|
Telemedicine |
Telemedicine is the practice of medicine that uses technology to provide healthcare services to patients who are located far away (telehealth). |
(Chau & Hu, 2002) |
|
Infrastructure |
The persons, facilities, and buildings necessary to offer world-class healthcare are included in the concept of healthcare infrastructure. |
(Leslie et al., 2017) |
|
Health Care Performance |
It measured based on the perception of respondents regarding efficiency, staff satisfaction, and patient satisfaction. |
(Cleven et al., 2016) |
4.1 Demographic analysis
The demographic data of the research participants are shown in Table 2. It can be viewed that all respondents belong to public sector healthcare organization. The majority of hospitals (N=131, 32.75%) have age between six and ten years, followed by between sixteen and twenty years (N=122, 30.5%), eleven and fifteen years (N=105, 26.25%), more than twenty years (N=29, 7.25%), and less than five years (N=13, 3.2%). In terms of size, most respondents were from large organizations with number of employees more than hundred (N=181, 45.25%). Whereas, 150 (37.5%) and 69 (17.25%) respondents were from small and medium hospitals, respectively.
In the perspective of Jordanian society, the sample has a fairly balanced gender distribution with 114 female respondents (28.5%) and 286 male respondents (71.5%). The biggest group in terms of age distribution is between the ages of 36 and 45 (N=136, 34%), followed by those between the ages of 26 and 35 (113 respondents, 28.25%), 45 and above (91 respondents, 22.75%), and those under the age of 25 (N=60, 15%). A bachelor's degree is the most common level of education held by respondents (N=169, 42.25%), followed by a diploma (N=124, 31%), and a master's degree (N=100, 25%). Only seven of the respondents, or 1.75% of the sample, have a PhD. According to the data analysis, 33.75% of respondents (N=135) had experience of working in the current organization for between two to ten years, while 25.75% (N=103) had experience working for between eleven and twenty years. In contrast, 101 respondents (25.25%) have fewer than 1 years of experience, while 62 respondents (15.15%) have experience of more than 20 years.
Table 2. Demographic information
|
Demographic |
Frequencies |
Percentage (%) |
|
Type of Hospital |
|
|
|
Public |
400 |
100 |
|
Private |
0 |
0 |
|
Age of Hospital |
|
|
|
Less than 5 years |
13 |
3.2 |
|
6-10 |
131 |
32.75 |
|
11-15 |
105 |
26.25 |
|
16-20 |
122 |
30.5 |
|
20 and above |
29 |
7.25 |
|
No. of Employees |
|
|
|
Between 6 to 20 (small) |
150 |
37.50 |
|
Between 21 to 100 (Medium) |
69 |
17.25 |
|
More than 100 (Large) |
181 |
45.25 |
|
Gender |
|
|
|
Male |
286 |
71.5 |
|
Female |
114 |
28.5 |
|
Age |
|
|
|
Less than 25 |
60 |
15 |
|
26-35 |
113 |
28.25 |
|
36-45 |
136 |
34 |
|
45 and above |
91 |
22.75 |
|
Academic Qualification |
|
|
|
Diploma |
124 |
31 |
|
Bachelor Degree |
169 |
42.25 |
|
Master Degree |
100 |
25 |
|
PhD Degree |
7 |
1.75 |
|
Exp in this organization |
|
|
|
Less than 1 years |
101 |
25.25 |
|
2-10 |
135 |
33.75 |
|
11-20 |
103 |
25.75 |
|
More than 20 years |
62 |
15.15 |
This study used the Partial Least Squares Structural Equation Modelling (PLS-SEM) approach as a multivariate analytic method to achieve its research objectives. In particular, SmartPLS was used to carry out the two-stage SEM analysis technique [68]. The validity and reliability of the instrument were evaluated using the measurement model, and assumed relationships were evaluated using the structural model. The significance of the coefficients and loadings were evaluated in the structural model using a bootstrapping method with 5000 resamples.
4.2 Measurement model
This study's first focus was on assessing the measurement model in order to confirm the validity and reliability of the measurements. To be more precise, the convergent and discriminant validities of the constructs were evaluated to assure their validity, and the internal consistency of the constructs was checked to ensure their reliability. The validity and reliability of the constructs were assessed using the following methodologies. This study conducted reliability tests to examine the internal consistency of the constructs. To ensure the validity of the constructs, this study evaluated the loadings and internal consistency of the indicators. All observed variables have acceptable outer loading levels ranging from 0.631 to 0.927, indicating satisfactory reliability of the items as shown in Table 3 [69]. The assessment of internal consistency and reliability is a crucial step. This study employed Cronbach's alpha and the Composite Reliability Index to test the internal consistency, Cronbach alpha values for the constructs range from 0.805 to 0.978, meeting the cut-off point of 0.7 [70].
Criticism has been made against the use of Cronbach's Alpha as a tool to assess reliability, with some scholars arguing that it underestimates actual reliability. As a result, the Composite Reliability Index was proposed by McNeish [71] as a more accurate measure to assess whether the specific indicators are adequate for representing the various structures. In order to establish appropriate internal consistency, the composite reliability should be greater than 0.7, as suggested by Barry et al. [70]. The composite reliability for each group of data exceeded the minimum cut-off value of 0.7, with a range of 0.860 to 0.980. These findings support the assertion that the required level of construct reliability has been achieved in the measurement model.
Table 3. Internal consistency reliability analysis
|
Constructs |
Items |
Indicator Reliability |
Internal Consistency |
|
|
Outer Loadings>0.5 |
Cronbach Alpha > 0.7 |
Composite Reliability >0.6 |
||
|
COVID-19 (COV) |
1 |
0.824 |
0.859 |
0.890 |
|
2 |
0.693 |
|||
|
3 |
0.650 |
|||
|
4 |
0.839 |
|||
|
5 |
0.747 |
|||
|
6 |
0.697 |
|
|
|
|
7 |
0.659 |
|
|
|
|
Telemedicine (TEL) |
1 |
0.888 |
0.950 |
0.958 |
|
2 |
0.855 |
|||
|
3 |
0.777 |
|||
|
4 |
0.876 |
|||
|
5 |
0.900 |
|
|
|
|
6 |
0.850 |
|
|
|
|
7 |
0.777 |
|
|
|
|
8 |
0.839 |
|
|
|
|
9 |
0.848 |
|
|
|
|
Innovation (INN) |
1 |
0.702 |
0.805 |
0.860 |
|
2 |
0.738 |
|||
|
3 |
0.763 |
|||
|
4 |
0.768 |
|||
|
5 |
0.658 |
|||
|
6 |
0.631 |
|||
|
Infrastructure (INF) |
1 |
0.910 |
0.978 |
0.980 |
|
2 |
0.914 |
|||
|
3 |
0.912 |
|||
|
4 |
0.903 |
|||
|
5 |
0.893 |
|||
|
6 |
0.906 |
|||
|
7 |
0.916 |
|||
|
8 |
0.927 |
|||
|
9 |
0.906 |
|||
|
10 |
0.859 |
|||
|
11 |
0.855 |
|||
|
12 |
0.864 |
|||
|
Hospital Management Performance (HP) |
1 |
0.747 |
0.881 |
0.907 |
|
2 |
0.765 |
|||
|
3 |
0.759 |
|||
|
4 |
0.768 |
|||
|
5 |
0.775 |
|
|
|
|
6 |
0.723 |
|
|
|
|
7 |
0.806 |
|
|
|
The degree to which each item accurately captures the construct in comparison to other latent variables is known as convergent validity [72]. This study computed the Average Variance Extracted (AVE) using the PLS technique in the SmartPLS software to assess convergent validity. The lowest AVE value of 0.507 and AIS infrastructure has the highest AVE value of 0.807. Among others, COVID-19, telemedicine, and hospital performance exhibited AVE values of 0.538, 0.717, and 0.583, respectively, which means all account for more than 50% of the variation. As a result, the findings imply that the measurement model exhibits a sufficient amount of convergent validity (Table 4).
Table 4. Convergent validity results
|
Constructs |
Convergent Validity (AVE > 0.5) |
|
COVID-19 |
0.538 |
|
Telemedicine |
0.717 |
|
Innovation |
0.507 |
|
Infrastructure |
0.807 |
|
Hospital Management Performance |
0.583 |
Table 5. HTMT results
|
COV |
HP |
INF |
INN |
TEL |
|
|
COV |
|||||
|
HP |
0.354 |
||||
|
INF |
0.888 |
0.364 |
|||
|
INN |
0.576 |
0.602 |
0.43 |
||
|
TEL |
0.517 |
0.442 |
0.408 |
0.604 |
To ensure that items measure the intended concepts and not other related constructs, discriminant validity of the model was assessed in this study. By looking at the correlations between items measuring various constructs, discriminant validity—which assesses how well a concept is distinct from other constructs—is examined [73]. In this work, the model's discriminant validity was assessed using the HTMT method. According to Henseler et al. [74], the HTMT, or the ratio of between-trait correlations to within-trait correlation, indicates issues with discriminant validity when it is over 0.9. None of the constructions surpassed the HTMT threshold level, the result of HTMT of this study is mentioned in Table 5.
The bootstrapping approach is used to determine the importance of each path link in the structural model, and the findings are shown in Table 6. Through repeated random sampling with replacement from the original sample, a bootstrap sample is created, and standard errors are obtained for hypothesis testing [70]. Chin [75] suggests using 1000 resamples while bootstrapping. Using the SmartPLS bootstrapping technique, 4 construct-specific direct relationships in total are evaluated first in this work. T-statistics are generated for each path to determine the significance level. Two-tailed test, 0.05 threshold of significance, and 5,000 subsamples are the parameters for the bootstrapping procedure. According to Ramayah et al. [73], the critical values for the two-tailed test at a significance level of 1% (p-value 0.01), 5% (p-value 0.05), and 10% (p-value 0.1) are 2.58, 1.96, and 1.38, respectively.
The coefficients in Table 2 have standardised values that range from -0.222 to 0.432, roughly between +1 and -1, showing a stronger association when the coefficients are closer to 1 and a weaker relationship when they are closer to zero [70]. The study discovered that COVID-19 situation has a significant and negative effect on hospital performance (H1) at the 5% level (β=-0.222, t=2.48, p=0.013). In contrast, telemedicine has a significant and positive impact on hospital performance (H2) at 5% level of significance (β=0.137, t=2.04, p=0.042). Moreover, infrastructure (β=0.432, t=3.191, p=0.002) and innovation (β=0.367, t=6.176, p<0.01) are positively related with hospital performance (H3 & H4) at the 1% level of significance. These findings show how these factors directly affect hospital management performance in Jordan. This study further analyses the moderating role of telemedicine, infrastructure, and innovation in the latter section to further explore its research objectives.
Table 6. Structural model results
|
Relationship |
BETA |
LL |
UL |
T-Value |
Sig |
Effect Size |
VIF |
|
COV -> HP |
-0.222 |
-0.44 |
-0.085 |
2.480 |
0.013 |
Small |
1.026 |
|
INF -> HP |
0.432 |
0.200 |
0.738 |
3.191 |
0.002 |
Small |
1.139 |
|
INN -> HP |
0.367 |
0.249 |
0.487 |
6.176 |
0.000 |
Small |
1.668 |
|
TEL -> HP |
0.137 |
0.004 |
0.258 |
2.037 |
0.042 |
Small |
1.577 |
5.1 Moderation analysis
Subsequently, this research delves into the exploration of hypothesized relationships through the utilization of moderation analysis. A moderating variable, as defined by Barry et al. [70], is a construct that influences the connection between explanatory and outcome variables. In the context of this study, telemedicine, infrastructure, and innovation are incorporated as moderating variables to assess their influence on the direct impact of COVID-19 on hospital performance. The moderation analysis is conducted using SmartPLS to ascertain moderating effects. Thus, a total of three hypotheses are examined to investigate the moderating influence of these variables on the adverse impact of COVID-19 on hospital management performance.
In this context, a novel interactive variable is formed by multiplying the indicators of independent and moderating variables, as described by Ramayah et al. [73]. As an example, to examine the moderating influence of telemedicine, innovation, and infrastructure on the relationship between the COVID-19 crisis and hospital performance, this study generated three interaction variables by multiplying COVID-19 with telemedicine, innovation, and infrastructure, respectively. The findings of the moderation analysis conducted using the bootstrapping approach are displayed in Table 7. The results indicate that telemedicine (β = 0.125, t = 3.91, p <0.01) and infrastructure (β = 0.071, t = 3.58, p <0.01) play a significant and positive moderating role in influencing the impact of the COVID-19 crisis on hospital management performance. Conversely, the analysis reveals insignificant coefficients for the moderating effect of innovation on the relationship between COVID-19 and hospital performance. As a result, this study accepts two hypotheses pertaining to the moderating influence of telemedicine and infrastructure in mitigating the negative consequences of COVID-19 on hospital performance. However, the hypothesis related to the moderating role of innovation in the impact of COVID-19 on hospital performance is rejected.
Table 7. Moderation results
|
Moderators |
LL |
UL |
T-value |
P-value |
Decision |
|
TEL*COV -> HP |
0.092 |
0.184 |
3.907 |
0.00 |
Supported |
|
INN*COV -> HP |
-0.243 |
0.147 |
1.196 |
0.232 |
Not Supported |
|
INF*COV -> HP |
0.056 |
0.132 |
3.581 |
0.00 |
Supported |
The primary focus of this research revolves around examining how the COVID-19 crisis has affected the management performance of the healthcare sector in Jordan. Specifically, the study aims to investigate the direct impact of various factors on healthcare management performance. Moreover, it seeks to identify key factors that could potentially play a crucial role in mitigating the adverse consequences of similar situations in the future. Given the significant ramifications of the recent pandemic, there is a growing concern among authorities regarding the need to be better prepared for such circumstances going forward.
This study argues that the COVID-19 pandemic has had a profound negative impact on hospital performance in Jordan. One of the key reasons is the overwhelming increase in patient load. The surge in COVID-19 cases has led to a substantial influx of patients seeking medical care, resulting in overcrowded hospitals and resource constraints. The limited availability of essential resources such as beds, ventilators, PPE, and medical supplies has further strained the healthcare system. Moreover, the pandemic has presented significant staffing challenges. Healthcare professionals have faced long working hours, high levels of stress, and increased risk of contracting the virus themselves. Staff shortages have emerged as a result of healthcare workers falling ill or needing to quarantine, placing additional strain on hospitals' ability to deliver quality care. Another study by Al-Tammemi [76] examined the impact of COVID-19 on the healthcare sector in Jordan, focusing on hospital management challenges. The research highlighted resource shortages, including beds, ventilators, and personal protective equipment, which significantly affected hospitals' ability to provide adequate care. The study emphasized the importance of strengthening the healthcare infrastructure and implementing proactive measures to improve hospital management performance. Furthermore, Abuhammad [13] conducted a study exploring the challenges faced by healthcare workers in Jordan during the pandemic. The research highlighted the significant psychological impact on healthcare professionals, including increased stress, anxiety, and burnout. These psychological burdens affected decision-making processes and teamwork, ultimately impacting hospital management performance.
The second aim of this study is to examine the direct effects of telemedicine, innovation, and infrastructure on healthcare management performance. To achieve this objective, three hypotheses are formulated. The results demonstrate that all three variables exhibit a significant and positive direct influence on hospital management performance. This indicates the importance of these factors in bolstering the capacity of hospitals, particularly during challenging circumstances. The evidence strongly supports the notion that telemedicine, innovation, and infrastructure play vital roles in enhancing hospital management performance. Consequently, all three hypotheses formulated for this objective are accepted, confirming the significant relationships between telemedicine, innovation, infrastructure, and improved hospital performance.
Previous recent literature has also highlighted the positive impact of telemedicine, innovation, and infrastructure on healthcare management performance in Jordan [77-79]. These factors have been identified as important contributors to improving the quality of healthcare services, enhancing efficiency, and addressing challenges faced by the healthcare system. Most importantly, telemedicine has emerged as a valuable tool in healthcare management, particularly during the COVID-19 pandemic. Vadivel et al. [77] has explored the use of telemedicine in Jordan and found that it has positively influenced healthcare management performance. Telemedicine enables remote consultations, monitoring, and follow-ups, reducing the need for in-person visits and allowing healthcare professionals to reach patients in remote areas. This technology has improved access to healthcare services, increased efficiency, and enhanced patient satisfaction.
The third objective of this study is to explore the moderating effect of telemedicine on the relationship between COVID-19 and hospital management performance. The findings of this study indicate a significant and positive moderating role of telemedicine in the influence of the COVID-19 crisis on healthcare management performance. This suggests that when telemedicine is utilized to a high extent, it has the potential to alleviate the challenges and difficulties faced in vulnerable situations caused by the pandemic. Recent research has also provided evidence of the significant role of telemedicine in the negative impact of COVID-19 on healthcare management performance in Jordan [80, 81]. The COVID-19 pandemic has posed unprecedented challenges to the healthcare sector, including increased patient volume, resource limitations, and the need for effective management strategies. Telemedicine, which involves the use of technology to provide remote healthcare services, has emerged as a crucial tool in mitigating the negative impact of the pandemic on healthcare management performance. Studies have shown that the implementation of telemedicine has played a significant role in addressing these challenges and improving overall healthcare outcomes around the globe [42, 44, 46].
The subsequent aim of this study is to examine the moderating effect of innovation on the relationship between COVID-19 and healthcare management performance. A hypothesis is formulated, suggesting a significant moderating role of innovation in mitigating the impact of the COVID-19 pandemic on hospital performance. Although previous recent research has shown that innovation plays a significant role in enhancing healthcare management performance [54, 55]. However, in the context of the COVID-19 crisis in Jordan, the findings of this study indicate an insignificant moderation effect of innovation on the negative impact of the pandemic on healthcare management performance. This suggests that despite the importance of innovation in normal circumstances, it may not have a significant mitigating effect on the challenges posed by the COVID-19 pandemic in the Jordanian healthcare sector. Several factors could contribute to this result. Firstly, the unprecedented nature of the pandemic may have overwhelmed the capacity of innovation to effectively address the challenges faced by healthcare management. Likewise, the rapid and unpredictable spread of the virus, coupled with the overwhelming influx of patients, may have limited the effectiveness of innovative strategies in mitigating the negative impact on healthcare management performance.
The last objective of this study focuses on examining the moderating influence of infrastructure on the relationship between COVID-19 and healthcare management performance. For instance, a study by Alryalat et al. [78] emphasized the importance of infrastructure, such as adequate physical facilities, medical equipment, and technology, in ensuring the efficient functioning of healthcare systems. They found that healthcare facilities with better infrastructure were better equipped to handle challenges and provide quality care during emergencies. Likewise, various research articles [58, 60, 61] have explored the impact of infrastructure on healthcare resilience during the COVID-19 pandemic. They revealed that healthcare organizations with robust infrastructure, including well-equipped hospitals, advanced technology systems, and efficient supply chains, were better prepared to manage the crisis effectively.
Theoretically, this study contributes to the resource-based view by proposing the moderating roles of telemedicine and infrastructure in the adverse impact of COVID-19 crisis on healthcare management performance. The significant moderating roles of telemedicine and healthcare infrastructure in mitigating the adverse impact of COVID-19 on healthcare management performance in Jordan have important theoretical implications within the context of resource-based theory. According to resource-based theory, organizations that possess and effectively utilize valuable and rare resources are more likely to achieve a competitive advantage and superior performance. Its significant moderating role suggests that healthcare organizations with higher levels of telemedicine usage have a better capacity to adapt to the challenges posed by COVID-19, leading to improved management performance. This aligns with resource-based theory, as telemedicine represents a valuable and unique resource that provides a competitive advantage by enhancing the organization's ability to respond to crisis situations.
Practically, this study also offers various practical implications for the different stakeholders. The finding that COVID-19 negatively impacts healthcare management performance in Jordan provides insights into the specific challenges faced by the healthcare sector during a pandemic. It highlights the need for further research to understand the resilient mechanism mitigating COVID-19 effects on healthcare management performance, including its impact on resources, processes, and decision-making. Likewise, the finding that COVID-19 negatively impacts healthcare management performance also calls for practical interventions to mitigate the adverse effects. Healthcare organizations and authorities should prioritize implementing strategies to ensure the availability of necessary resources, adequate staffing, and appropriate protocols to manage crises effectively.
Overall, this study suggests Jordanian authorities and healthcare management to devise effective practical strategies for mitigating the negative impact of similar future crises. Specifically, healthcare organizations should focus on strengthening telemedicine capabilities, fostering a culture of innovation, and investing in resilient infrastructure to enhance the ability to manage and respond to such crises effectively. The identification of telemedicine and healthcare infrastructure as crucial moderating factors underscores the importance of investing in and prioritizing these resources within the healthcare sector. Policymakers and healthcare administrators can utilize these findings to inform decision-making processes and allocate resources effectively. For example, increased investment in telemedicine technology and infrastructure can enhance healthcare organizations' preparedness and response capabilities during times of crisis, improving the overall management performance. Moreover, healthcare professionals and practitioners can benefit by adopting and integrating these resources into their practices, enabling better healthcare service delivery, remote consultations, and enhanced patient care. This study emphasizes the importance of adapting to emerging technologies and strengthening infrastructure to ensure the continuity and quality of healthcare services, especially during times of crisis such as the COVID-19 pandemic.
While this study has made valuable contributions, it is important to acknowledge its limitations and provide recommendations for future research. Firstly, this study focuses specifically on the public healthcare sector in Jordan, which may limit the generalizability of the findings. Future researchers are encouraged to consider a broader target population, including private healthcare sectors, to provide more comprehensive and generalizable insights. Likewise, it is recommended that future studies delve into specific regions within Jordan that may exhibit varying levels of vulnerabilities. By examining different regions, researchers can gain a deeper understanding of the contextual factors that influence the impact of COVID-19 on healthcare management performance. This regional focus can contribute to more tailored and targeted interventions to address specific challenges faced by healthcare organizations in different areas. In addition, this study serves as a single-case study of Jordan, which may limit the generalizability of the findings to a global context. Future research should aim to include a larger sample size comprising multiple countries, allowing for cross-country comparisons and providing more comprehensive implications for the global healthcare community. By incorporating a diverse range of countries, researchers can identify common patterns, differences, and best practices in managing healthcare crises, including the impact of COVID-19 on healthcare management performance.
Moreover, this study adopts a quantitative research methodology, providing valuable insights into the impact of crises and their adversities on healthcare management performance. However, it is recommended that future studies complement these quantitative findings with qualitative methods to gain a deeper understanding of the nuances and intricacies of healthcare crises. By incorporating qualitative approaches, researchers can explore the constraints and specific requirements faced by healthcare organizations in each environment, offering a more comprehensive perspective. Qualitative methods would enable researchers to delve into the experiences and perspectives of healthcare staff and management, capturing their unique insights and providing a rich contextual understanding of the challenges they face during crises. This qualitative lens can shed light on the intricacies of decision-making processes, organizational dynamics, and the effectiveness of strategies employed by healthcare organizations in managing crises. Therefore, future studies are encouraged to adopt qualitative research methods alongside quantitative approaches to capture the human element and contextual factors that influence healthcare management performance during crises. By doing so, researchers can provide crucial implications that encompass a different perspective, offering a more holistic understanding of the challenges and opportunities faced by healthcare organizations in times of crisis.
Furthermore, this study emphasizes the significance of telemedicine and infrastructure as moderating factors that effectively mitigate the adversities arising from the COVID-19 crisis. Considering these findings, future studies are encouraged to broaden their scope and examine a wider range of resource-based variables that have the potential to play a crucial role in managing healthcare operations during periods of vulnerability. Expanding the investigation to include additional resource-based variables can provide a more comprehensive understanding of the factors that contribute to successful healthcare management during crises. By exploring a broader set of resources, researchers can identify and evaluate the effectiveness of various strategies and interventions that may enhance healthcare system resilience and responsiveness in the face of future challenges. Therefore, it is recommended that future studies incorporate an extensive array of resource-based variables, such as human resources, financial resources, technological resources, and organizational capabilities, to explore their potential as mitigating factors in managing healthcare operations during vulnerable times. Such an approach will enable a more holistic examination of the multifaceted nature of resource-based interventions and their impact on healthcare management performance.
[1] Jalghoum, Y., Tahtamouni, A., Khasawneh, S., Al-Madadha, A. (2021). Challenges to healthcare information systems development: The case of Jordan. International Journal of Healthcare Management, 14(2): 447-455. https://doi.org/10.1080/20479700.2019.1658159
[2] Mitias, A. (2021). The blue state: UNRWA's transition from relief to development in providing education to palestinian refugees in Jordan. Honors Theses. University of Mississippi.
[3] Al-Rimmawi, H., Kittaneh, M. (2022). Fate of palestinian refugee camps in syria after the so called arab spring. GeoJournal, 87(4): 3077-3089. https://doi.org/10.1007/s10708-021-10419-0
[4] Pinto, D.M. (2021). VitalCoViD Platform: web-based telehealth system for real-time monitoring of COVID-19 patients at home using wearable health devices. Doctoral dissertation, Universidade do Porto (Portugal).
[5] Harahsheh, A.A., Houssien, A.A., Alshurideh, M.T., Mohammad, A. (2021). The effect of transformational leadership on achieving effective decisions in the presence of psychological capital as an intermediate variable in private Jordanian universities in light of the corona pandemic. The Effect of Coronavirus Disease (COVID-19) on Business Intelligence, 221-243. https://doi.org/10.1007/978-3-030-67151-8_13
[6] Zhang, S.X., Liu, J., Jahanshahi, A.A., Nawaser, K., Yousefi, A., Li, J., Sun, S. (2020). At the height of the storm: Healthcare staff’s health conditions and job satisfaction and their associated predictors during the epidemic peak of COVID-19. Brain, Behavior, and Immunity, 87: 144-146. https://doi.org/10.1016/j.bbi.2020.05.010
[7] Abu Mansour, S.I., Abu Shosha, G.M. (2022). Experiences of first-line nurse managers during COVID-19: A Jordanian qualitative study. Journal of Nursing Management, 30(2): 384-392. https://doi.org/10.1111/jonm.13530
[8] Hussein, A.M.A., Mohammad, A.M., Alheet, A., Joma, M.H.A., Lehyeh, S.A. (2023). Relationships between human resource management practices, employee satisfaction, service quality, and employee service behavior in the hotel industry. Problems and Perspectives in Management, 21(1): 242-252. https://doi.org/10.21511/ppm.21(1).2023.21
[9] Vrontis, D., El Chaarani, H., El Abiad, Z., El Nemar, S., Yassine Haddad, A. (2022). Managerial innovative capabilities, competitive advantage and performance of healthcare sector during COVID-19 pandemic period. Foresight, 24(3/4): 504-526. https://doi.org/10.1108/FS-02-2021-0045
[10] Mohammad, A., Menhat, M., Zaideen, I.M.M., Saadon, M.S.I. (2023). Leadership style and its influence on employee performance and retention in employee engagement mediation: Evidence from Jordan's petroleum retailing sector. International Journal of Procurement Management, 18(4): 437-469. https://doi.org/10.1504/IJPM.2022.10050345
[11] Wherton, J., Greenhalgh, T., Hughes, G., Shaw, S.E. (2022). The role of information infrastructures in scaling up video consultations during COVID-19: Mixed methods case study into opportunity, disruption, and exposure. Journal of Medical Internet Research, 24(11): e42431.
[12] Alzubi, E., Akkerman, R. (2022). Sustainable supply chain management practices in developing countries: An empirical study of Jordanian manufacturing companies. Cleaner Production Letters, 2: 100005. https://doi.org/10.1016/j.clpl.2022.100005
[13] Abuhammad, S. (2020). Barriers to distance learning during the COVID-19 outbreak: A qualitative review from parents’ perspective. Heliyon, 6(11): E05482. https://doi.org/10.1016/j.heliyon.2020.e05482
[14] Abufaraj, M., Xu, T., Cao, C., Siyam, A., Isleem, U., Massad, A., Soria, F., Shariat, S.F., Sutcliffe, S., Yang, L. (2021). Prevalence and trends in urinary incontinence among women in the United States, 2005–2018. American Journal of Obstetrics and Gynecology, 225(2): 166.e1-166.e12. https://doi.org/10.1016/j.ajog.2021.03.016
[15] Jum'a, L., Zimon, D., Madzik, P. (2023). Impact of big data technological and personal capabilities on sustainable performance on Jordanian manufacturing companies: The mediating role of innovation. Journal of Enterprise Information Management. https://doi.org/10.1108/JEIM-09-2022-0323
[16] Alghafary, N.A., Diabat, K.W., Abuhawileh, M.A.H. (2021). The degree of availability of crisis management elements in the boards of directors of Jordanian football sport clubs in light of the coronavirus (COVID-19) pandemic. International Journal of Human Movement and Sports Sciences, 9(4): 781-790.
[17] Gerada, C., Jones, R. (2014). Surgeons and mental illness: A hidden problem? BMJ, 348.
[18] Sirois, F.M., Owens, J. (2021). Factors associated with psychological distress in health-care workers during an infectious disease outbreak: A rapid systematic review of the evidence. Frontiers in Psychiatry, 11: 589545. https://doi.org/10.3389/fpsyt.2020.589545
[19] Wang, C., Horby, P.W., Hayden, F.G., Gao, G.F. (2020). A novel coronavirus outbreak of global health concern. The Lancet, 395(10223): 470-473. https://doi.org/10.1016/S0140-6736(20)30185-9
[20] Chirico, F., Gómez-Mejia, L.R., Hellerstedt, K., Withers, M., Nordqvist, M. (2020). To merge, sell, or liquidate? Socioemotional wealth, family control, and the choice of business exit. Journal of Management, 46(8): 1342-1379. https://doi.org/10.1177/0149206318818723
[21] Ayanian, J.Z. (2020). Mental health needs of health care workers providing frontline COVID-19 care. In JAMA Health Forum, 1(4): e200397-e200397. https://doi.org/10.1001/jamahealthforum.2020.0397
[22] Tahan, H.M. (2020). Essential case management practices amidst the novel coronavirus disease 2019 (COVID-19) crisis: Part 2: End-of-life care, workers' compensation case management, legal and ethical obligations, remote practice, and resilience. Professional Case Management, 25(5): 267–284. https://doi.org/10.1097/NCM.0000000000000455
[23] Xiao, X., Newman, C., Buesching, C.D., Macdonald, D.W., Zhou, Z.M. (2021). Animal sales from Wuhan wet markets immediately prior to the COVID-19 pandemic. Scientific Reports, 11(1): 1-7, https://doi.org/10.1038/s41598-021-91470-2
[24] Ghanemi, A., Yoshioka, M., St-Amand, J. (2020). Will an obesity pandemic replace the coronavirus disease-2019 (COVID-19) pandemic? Medical Hypotheses, 144: 110042. https://doi.org/10.1016/j.mehy.2020.110042
[25] Zhong, B., Huang, Y., Liu, Q. (2021). Mental health toll from the coronavirus: Social media usage reveals Wuhan residents’ depression and secondary trauma in the COVID-19 outbreak. Computers in Human Behavior, 114: 106524. https://doi.org/10.1016/j.chb.2020.106524
[26] Keeley, A.J., Evans, C., Colton, H., Ankcorn, M., Cope, A., Bennett, T., Giri, P., de Silva, T.I., Raza, M. (2020). Roll-out of SARS-CoV-2 testing for healthcare workers at a large NHS foundation trust in the United Kingdom, March 2020. Eurosurveillance, 25(14): 2000433. https://doi.org/10.2807/1560-7917.ES.2020.25.14.2000433
[27] Logishetty, K., Subramanyam, S. (2017). Adopting and sustaining a Virtual Fracture Clinic model in the District Hospital setting–A quality improvement approach. BMJ Quality Improvement Reports, 6(1): u220211-w7861. http://doi.org/10.1136/bmjquality.u220211.w7861
[28] Wadali, J.S., Sood, S.P., Kaushish, R., Syed-Abdul, S., Khosla, P.K., Bhatia, M. (2020). Evaluation of free, open-source, web-based DICOM viewers for the Indian national telemedicine service (eSanjeevani). Journal of Digital Imaging, 33: 1499-1513. https://doi.org/10.1007/s10278-020-00368-4
[29] Sandars, J., Correia, R., Dankbaar, M., de Jong, P., Goh, P. S., Hege, I., Masters, K., Oh, S.Y., Patel, R., Premkumar, K., Webb, A., Pusic, M. (2020). Twelve tips for rapidly migrating to online learning during the COVID-19 pandemic. MedEdPublish, 9: 82. https://doi.org/10.15694/mep.2020.000082.1
[30] Naseri, H., Jahanbakhsh, H., Hosseini, P., Nejad, F.M. (2020). Designing sustainable concrete mixture by developing a new machine learning technique. Journal of Cleaner Production, 258: 120578. https://doi.org/10.1016/j.jclepro.2020.120578
[31] Davis, T.M., Barden, C., Dean, S., et al. (2016). American telemedicine association guidelines for TeleICU operations. Telemedicine and e-Health, 22(12): 971-980. https://doi.org/10.1089/tmj.2016.0065
[32] Uscher-Pines, L., Pines, J., Kellermann, A., Gillen, E., Mehrotra, A. (2013). Emergency department visits for nonurgent conditions: Systematic literature review. The American Journal of Managed Care, 19(1): 47-59.
[33] Woodside, J.M., Augustine Jr, F.K., Giberson, W. (2017). Blockchain technology adoption status and strategies. Journal of International Technology and Information Management, 26(2): 65-93. https://doi.org/10.58729/1941-6679.1300
[34] Moore, B., Woodcock, S. (2017). Resilience, bullying, and mental health: Factors associated with improved outcomes. Psychology in the Schools, 54(7): 689-702. https://doi.org/10.1002/pits.22028
[35] Di Cerbo, A., Morales-Medina, J.C., Palmieri, B., Iannitti, T. (2015). Narrative review of telemedicine consultation in medical practice. Patient Preference and Adherence, 65-75. https://doi.org/10.2147/PPA.S61617
[36] Lepore, J. (2018). These truths: A history of the United States. WW Norton & Company.
[37] Destgeer, G., Ha, B.H., Park, J., Jung, J.H., Alazzam, A., Sung, H.J. (2015). Microchannel anechoic corner for size-selective separation and medium exchange via traveling surface acoustic waves. Analytical Chemistry, 87(9): 4627-4632. https://doi.org/10.1021/acs.analchem.5b00525
[38] Bawack, R.E., Kamdjoug, J.R.K. (2018). Adequacy of UTAUT in clinician adoption of health information systems in developing countries: The case of Cameroon. International Journal of Medical Informatics, 109: 15-22. https://doi.org/10.1016/j.ijmedinf.2017.10.016
[39] Farahani, B., Firouzi, F., Chang, V., Badaroglu, M., Constant, N., Mankodiya, K. (2018). Towards fog-driven IoT eHealth: Promises and challenges of IoT in medicine and healthcare. Future Generation Computer Systems, 78: 659-676. https://doi.org/10.1016/j.future.2017.04.036
[40] Mlcochova, P., Kemp, S.A., Dhar, M.S., et al. (2021). SARS-CoV-2 B. 1.617. 2 Delta variant replication and immune evasion. Nature, 599(7883): 114-119. https://doi.org/10.1038/s41586-021-03944-y
[41] Sparkes, A.H., Caney, S., Chalhoub, S., Elliott, J., Finch, N., Gajanayake, I., Langston, C., Lefebvre, H.P., White, J., Quimby, J. (2016). ISFM consensus guidelines on the diagnosis and management of feline chronic kidney disease. Journal of Feline Medicine and Surgery, 18(3): 219-239. https://doi.org/10.1177/1098612X16631234
[42] Shin, H., Lee, J.H., Moon, C.K., Huh, J.S., Sim, B., Kim, J.J. (2016). Sky-blue phosphorescent OLEDs with 34.1% external quantum efficiency using a low refractive index electron transporting layer. Advanced Materials, 28(24): 4920-4925. https://doi.org/10.1002/adma.201506065
[43] Rogers, W.A., Mitzner, T.L. (2017). Envisioning the future for older adults: Autonomy, health, well-being, and social connectedness with technology support. Futures, 87: 133-139. https://doi.org/10.1016/j.futures.2016.07.002
[44] Hollander, J.E., Carr, B.G. (2020). Virtually perfect? Telemedicine for COVID-19. New England Journal of Medicine, 382(18): 1679-1681. https://doi.org/10.1056/nejmp2003539
[45] Kayyali, R., Peletidi, A., Ismail, M., Hashim, Z., Bandeira, P., Bonnah, J. (2017). Awareness and use of mHealth apps: A study from England. Pharmacy, 5(2): 33. https://doi.org/10.3390/pharmacy5020033
[46] Menhat, M., Yusuf, Y., Gunasekaran, A., Mohammad, A.M. (2022). Performance measurement framework for the oil and gas supply chain. Benchmarking: An International Journal. https://doi.org/10.1108/BIJ-11-2021-0704
[47] Hale, T., Angrist, N., Kira, B., Petherick, A., Phillips, T., Webster, S. (2020). Variation in government responses to COVID-19.
[48] Hussain, A., Bhowmik, B., do Vale Moreira, N.C. (2020). COVID-19 and diabetes: Knowledge in progress. Diabetes Research and Clinical Practice, 162: 108142. https://doi.org/10.1016/j.diabres.2020.108142
[49] Radzikowska, U., Ding, M., Tan, G., et al. (2020). Distribution of ACE2, CD147, CD26, and other SARS-CoV-2 associated molecules in tissues and immune cells in health and in asthma, COPD, obesity, hypertension, and COVID-19 risk factors. Allergy, 75(11): 2829-2845. https://doi.org/10.1111/all.14429
[50] Gatto, M., Bertuzzo, E., Mari, L., Miccoli, S., Carraro, L., Casagrandi, R., Rinaldo, A. (2020). Spread and dynamics of the COVID-19 epidemic in Italy: Effects of emergency containment measures. Proceedings of the National Academy of Sciences, 117(19): 10484-10491. https://doi.org/10.1073/pnas.2004978117
[51] Xie, G., Paik, Y. (2019). Cultural differences in creativity and innovation: Are Asian employees truly less creative than western employees? Asia Pacific Business Review, 25(1): 123-147. https://doi.org/10.1080/13602381.2018.1535380
[52] Hofstede, G. (1984). Culture's consequences: International differences in work-related values (Vol. 5). sage.
[53] Morris, W., Leung, B., Furukawa, H., Yaghi, O.K., He, N., Hayashi, H., Houndonougbo, B., Asta, M., Laird, B.B., Yaghi, O.M. (2010). A combined experimental− computational investigation of carbon dioxide capture in a series of isoreticular zeolitic imidazolate frameworks. Journal of the American Chemical Society, 132(32): 11006-11008. https://doi.org/10.1021/ja104035j
[54] Wang, P.W., Ahorsu, D.K., Lin, C.Y., Chen, I.H., Yen, C.F., Kuo, Y.J., Griffiths, M.D., Pakpour, A.H. (2021). Motivation to have COVID-19 vaccination explained using an extended protection motivation theory among university students in China: the role of information sources. Vaccines, 9(4): 380. https://doi.org/10.3390/vaccines9040380
[55] Tareq, M.S., Rahman, T., Hossain, M., Dorrington, P. (2021). Additive manufacturing and the COVID-19 challenges: An in-depth study. Journal of Manufacturing Systems, 60: 787-798. https://doi.org/10.1016/j.jmsy.2020.12.021
[56] Nambisan, S., Wright, M., Feldman, M. (2019). The digital transformation of innovation and entrepreneurship: Progress, challenges and key themes. Research Policy, 48(8): 103773. https://doi.org/10.1016/j.respol.2019.03.018
[57] Abu-Rumman, A., Al Shraah, A., Al-Madi, F., Alfalah, T. (2022). The impact of quality framework application on patients’ satisfaction. International Journal of Human Rights in Healthcare, 15(2): 151-165. https://doi.org/10.1108/IJHRH-01-2021-0006
[58] Seda, G., Parrish, J.S. (2019). Augmenting critical care capacity in a disaster. Critical Care Clinics, 35(4): 563-573, 10.1016/j.ccc.2019.06.007
[59] Iyengar, K., Bahl, S., Vaishya, R., Vaish, A. (2020). Challenges and solutions in meeting up the urgent requirement of ventilators for COVID-19 patients. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, 14(4): 499-501. https://doi.org/10.1016/j.dsx.2020.04.048
[60] Tortorella, G.L., Vergara, A.M.C., Garza-Reyes, J.A., Sawhney, R. (2020). Organizational learning paths based upon industry 4.0 adoption: An empirical study with Brazilian manufacturers. International Journal of Production Economics, 219: 284-294. https://doi.org/10.1016/j.ijpe.2019.06.023
[61] Hartmann, N.N., Lussier, B. (2020). Managing the sales force through the unexpected exogenous COVID-19 crisis. Industrial Marketing Management, 88: 101-111. https://doi.org/10.1016/j.indmarman.2020.05.005
[62] Al-Khrabsheh, A.A., Al-Bazaiah, S.A., Al-Khrabsheh, A.A., Alheet, A.F. (2022). The strategic role of human resources management in performing crisis management: The mediating role of organizational culture and human capital during Covid-19 (An Applied Study on the Jordanian Ministry of Health). Journal of Management Information and Decision Sciences, 25: 1-18.
[63] Ahorsu, D.K., Lin, C.Y., Marznaki, Z.H., H Pakpour, A. (2022). The association between fear of COVID-19 and mental health: The mediating roles of burnout and job stress among emergency nursing staff. Nursing Open, 9(2): 1147-1154. https://doi.org/10.1002/nop2.1154
[64] Yoon, E., Babar, A., Choudhary, M., Kutner, M., Pyrsopoulos, N. (2016). Acetaminophen-induced hepatotoxicity: A comprehensive update. Journal of Clinical and Translational Hepatology, 4(2): 131. https://doi.org/10.14218%2FJCTH.2015.00052
[65] Leslie, H.A., Brandsma, S.H., Van Velzen, M.J.M., Vethaak, A.D. (2017). Microplastics en route: Field measurements in the Dutch river delta and Amsterdam canals, wastewater treatment plants, North Sea sediments and biota. Environment International, 101: 133-142. https://doi.org/10.1016/j.envint.2017.01.018
[66] Chau, P.Y., Hu, P.J. (2002). Examining a model of information technology acceptance by individual professionals: An exploratory study. Journal of Management Information Systems, 18(4): 191-229. https://doi.org/10.1080/07421222.2002.11045699
[67] Cleven, A.H., Al Sannaa, G.A., Briaire-de Bruijn, I., et al. (2016). Loss of H3K27 tri-methylation is a diagnostic marker for malignant peripheral nerve sheath tumors and an indicator for an inferior survival. Modern Pathology, 29(6): 582-590. https://doi.org/10.1038/modpathol.2016.45
[68] Hair, J.F., Ringle, C.M., Sarstedt, M. (2011). PLS-SEM: Indeed a silver bullet. Journal of Marketing theory and Practice, 19(2): 139-152. https://doi.org/10.2753/MTP1069-6679190202
[69] Byrne, R.M. (2016). Counterfactual thought. Annual Review of Psychology, 67: 135-157. https://doi.org/10.1146/annurev-psych-122414-033249
[70] Barry, Hair, J.B., Rolph, E.A. (2010). Multivariate Data Analysis. New York: Macmillan: Pearson Prentice Hall.
[71] McNeish, D. (2017). Small sample methods for multilevel modeling: A colloquial elucidation of REML and the Kenward-Roger correction. Multivariate Behavioral Research, 52(5): 661-670. https://doi.org/10.1080/00273171.2017.1344538
[72] Urbach, N., Ahlemann, F. (2010). Structural equation modeling in information systems research using partial least squares. Journal of Information Technology Theory and Application (JITTA), 11(2): 2.
[73] Ramayah, T.J.F.H., Cheah, J., Chuah, F., Ting, H., Memon, M.A. (2018). Partial least squares structural equation modeling (PLS-SEM) using smartPLS 3.0. An updated guide and practical guide to statistical analysis. Kuala Lumpur, Malaysia: Pearson.
[74] Henseler, J., Ringle, C.M., Sarstedt, M. (2015). A new criterion for assessing discriminant validity in variance-based structural equation modeling. Journal of the Academy of Marketing Science, 43: 115-135. https://doi.org/10.1007/s11747-014-0403-8
[75] Chin, W.W. (2009). How to write up and report PLS analyses. In Handbook of Partial Least Squares: Concepts, Methods and Applications, pp. 655-690. https://doi.org/10.1007/978-3-540-32827-8_29
[76] Al-Tammemi, A.A.B. (2020). The battle against COVID-19 in Jordan: An early overview of the Jordanian experience. Frontiers in Public Health, 8: 188. https://doi.org/10.3389/fpubh.2020.00188
[77] Vadivel, R., Shoib, S., El Halabi, S., et al. (2021). Mental health in the post-COVID-19 era: Challenges and the way forward. General Psychiatry, 34(1): e100424. https://doi.org/10.1136%2Fgpsych-2020-100424
[78] Alryalat, S.A.S., Malkawi, L.W., Momani, S.M. (2019). Comparing bibliometric analysis using PubMed, Scopus, and Web of Science databases. JoVE (Journal of Visualized Experiments), 152: e58494. https://doi.org/10.3791/58494
[79] Alshourah, S. (2021). Total quality management practices and their effects on the quality performance of Jordanian private hospitals. Management Science Letters, 11(1): 67-76. http://doi.org/10.5267/j.msl.2020.8.029
[80] Shatnawi, N.J., Mesmar, Z., Al-Omari, G.A., Al-Sheyab, W., AlZoubi, N.A., Al-Ghazo, M., Hamouri, A., AL-Faori, I., Bani-Essa, A., Matalka, I., Khader., Y.S., Batieha, A. (2022). Compliance with safety measures and risk of COVID-19 transmission among healthcare workers. Future Science OA, 8(1): FSO762. https://doi.org/10.2144/fsoa-2021-0094
[81] Saddik, B., Al-Bluwi, N., Shukla, A., Barqawi, H., Alsayed, H.A.H., Sharif-Askari, N.S., Temsah, M.H., Bendardaf, R., Hamid, Q., Halwani, R. (2022). Determinants of healthcare workers perceptions, acceptance and choice of COVID-19 vaccines: A cross-sectional study from the United Arab Emirates. Human Vaccines & Immunotherapeutics, 18(1): 1-9. https://doi.org/10.1080/21645515.2021.1994300