Saeed Hussein Alhmoud*![]() | Husam Hussein Alhmoud
| Husam Hussein Alhmoud![]() | Khaled Hussein Alhmoud
| Khaled Hussein Alhmoud![]() | Anas Mohammad Bataineh
| Anas Mohammad Bataineh![]() | Çiğdem Çağnan
| Çiğdem Çağnan![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Pressure sores, also referred to as bed sores, are skin ulcers linked to coma that become a major concern when caring for critically ill patients in the intensive care unit who are immobile. Persistent pressure on specific body parts that arises from remaining in one spot for an extended period of time will undoubtedly damage the tissues, making the patient uncomfortable, resulting in long-term recovery time and treatment more difficult. Among other things, choosing the appropriate bed type is a crucial step in preventing the occurrence of these sores and ensuring that patients receive the healthcare they need. The purpose of the paper is to demonstrate how bed design can help comatose people experience fewer skin ulcers. The study examines the impact of various elements on ulcer risk reduction, including material selection, bed adjustability, pressure distribution, and patient repositioning techniques. Additionally, the study assesses the impact of the bed's caregiver-focused features, accessibility, mobility aid, and environmental control on patient outcomes and care quality. In order to provide the necessary practical design changes that will not only lower the rate of coma-associated skin ulcers but also increase patient satisfaction and facilitate caregiving, the current research effectively integrates the outlines of ergonomic bed models and the planned activity. Prototype tests showed a 42% reduction in sacral regional pressure (p<0.01) in a clinical trial involving 50 patients. In addition, the paper introduces the idea of smart beds as one of the cutting-edge technologies that will help patients better identify their movements and point out early pressure wound healing symptoms. The study emphasises how crucial comprehensive design is to accelerating patient recovery and lowering immobility-related complications in critical care environments.
ICU bed, patient comfort, ergonomic, coma-related skin ulcers, pressure ulcer prevention, nanocoating
Traditional ICU bed designs have historically been constructed primarily to guarantee acute care. For instance, they offer the potential for emergency accessibility, haemodynamic monitoring, and integration with life-support systems. The typical static mattresses and less flexible bed frames are the primary components needed only for the short-term treatment and are ineffective at performing the biomechanical tasks of prolonged immobilisation, as opposed to primarily using physiotherapeutic tactics to regulate pressure-related tissue damage. Therefore, the high-risk sacrum, heels, and occipital regions continue to be subjected to pressure ulcers, shear, and moisture, all of which lead to tissue ischaemia and the necrosis that follows [1, 2]. In addition to the clinical consideration, there is an ethical imperative to expedite the redesign of intensive care unit beds and spatial arrangements. The increasing acknowledgement of pressure ulcers as a "never event," a preventable harm that demonstrates the shortcomings in care quality, has further highlighted this [3].
In addition to being one of the most unmanageable and preventable ICU-related complications, pressure sores, also called bedsores, are typically injuries that are limited to a portion of the skin and even the tissue beneath it. They are brought on by prolonged exposure to pressure or shear forces. These patients are more likely to develop such sores, according to data from studies that present information about patients in a highly unconscious state, their bodies being immobile, and their reliance on machines. According to reports, 15–25% of critically ill patients in the intensive care unit experience pressure injuries; comatose patients are especially vulnerable because they are unable to move or communicate their discomfort [4]. This implies that these damages not only result in significant pain, which is obviously physical in nature, but also a greater healthcare burden, such as that brought on by extended hospital stays, elevated risks of infection, and correspondingly higher treatment expenses, all of which ultimately impede patient recovery and reduce hospital productivity.
Recent developments in biomedical equipment and healthcare construction have produced ICU bed systems that have the potential to improve care by combining patient, carer, and comfort safety. One of the most dangerous aspects of patient care is coma-induced pressure sores, which are brought on by prolonged immobility and inadequate body pressure distribution in intensive care units. These wounds are produced when persistent pressure results in blood flow obstruction, which causes tissue ischaemia and necrosis. This increases the severity of the case, length of hospital stay, and medical expenses. As it stands, the common intensive care unit beds lack the ergonomic features necessary to eliminate pressure irregularities and control the patients' strong repositioning. Emerging technologies, like smart beds with dynamic pressure redistribution and materials that regulate the microclimate, can help prevent and lessen the incidence of skin ulcers while also greatly easing the workload of medical personnel [5, 6]. Therefore, it is argued that moving ICU beds to make them easier for staff to use, for carers to handle, and for environmental controls can not only reduce the risk of patient-related sores but also indirectly lower the risk of ulcers by reducing needless patient manipulation and increasing adherence to preventive protocols [7]. It is still necessary to connect the staff's small technological advancements with the patient-centered healthcare system's ordering, which addresses many of the factors that contribute to coma-related skin ulcers, even though technological advancements are in the right direction.
While immobility is a shared risk factor for pressure ulcers across various patient populations, comatose patients present a distinct clinical challenge due to their complete lack of voluntary movement and inability to communicate discomfort or pain. These patients are entirely reliant on external care for repositioning, thermal regulation, and pressure redistribution, making them disproportionately susceptible to pressure injuries, especially in ICU settings [3].
According to international prevalence data, the incidence of pressure injuries in ICUs ranges from 15% to 25%, but among comatose patients, this rate often exceeds 30% due to prolonged unresponsiveness and deep sedation [1]. Furthermore, comatose patients are more likely to experience adverse outcomes such as tissue ischemia, infection, and extended hospitalization as a result of pressure ulcers, which not only compromise patient recovery but also increase the burden on healthcare systems.
To frame the scope of the study more clearly, we have now integrated a concise overview of the core design elements addressed in this research. These include:
Pressure Redistribution: The study evaluates advanced mattress materials (e.g., viscoelastic foams and honeycomb structures) and bed adjustability mechanisms (e.g., lateral tilting, elevation systems) designed to reduce prolonged pressure on high-risk zones such as the sacrum, heels, and occiput.
Microclimate Management: We assess features such as nanotechnology-enhanced waterproofing layers, ventilation systems, and phase-change materials that regulate temperature and moisture at the skin–mattress interface, critical in reducing maceration and microbial growth.
Ergonomics: Special consideration is given to caregiver-centered features, including modular adjustability, touchscreen controls, and smart feedback systems that reduce physical strain, enhance repositioning protocols, and improve care precision [6].
Combining the fields of design, material science, clinical care, and technology for the unconscious patients in the intensive care unit (ICU); the ultimate goal of this research is to be able to make pertinent and useful recommendations and evaluate them using an integrative approach to the Intensive Care Unit's (ICU) bed design and spatial layout. The primary concern of the study is how to prevent coma-induced pressure ulcers. This study discusses human factors, modern pressure relief techniques, and patient pain elimination. The scope includes the following important areas in Table 1.
Table 1. Critically assess essential aspects of ICU bed design
|
ICU Bed Design Feature |
Evaluation Criteria and Impact |
|
Mattress Materials |
Evaluation of pressure-relieving properties to minimize the risk of pressure ulcers. |
|
Bed Adjustability |
Examination of features such as elevation, tilt, and rotation mechanisms, which play a crucial role in redistributing pressure and reducing ulcer risks. |
|
Smart Bed Technologies |
Assessment of advanced systems such as smart beds that monitor pressure points and automatically adjust to alleviate pressure, improving patient outcomes. |
|
Waterproofing and Nanotechnology Integration |
Investigating how these materials can improve bed durability and hygiene. |
|
Vibration Mechanisms |
Analysis of vibrating elements between the bed base and mattress to enhance comfort and assist in pressure relief. |
|
Air Equalization Systems |
Evaluation of devices designed to balance air distribution within the bed, improving patient comfort. |
|
Air Vents on the Mattress Surface |
Study of air vents on the sponge side of ICU mattresses to improve airflow and reduce heat accumulation, contributing to pressure relief. |
|
Honeycomb-Shaped Sponge Design |
Investigation of sponge structures designed to optimize pressure distribution and enhance patient comfort. |
|
Technological Innovations in ICU Beds |
The study will delve into emerging technologies in ICU bed design, particularly those incorporating sensors for early detection of skin ulcers. These technologies will be analyzed for their effectiveness in preventing ulcers and improving patient care. |
|
Caregiver Ergonomics |
Evaluation of the physical demands on caregivers and how bed design impacts their ability to provide effective care. |
Through the integration of ICU bed design and patient care, the study seeks to improve pressure ulcers and patient recovery rates in patients in prolonged coma.
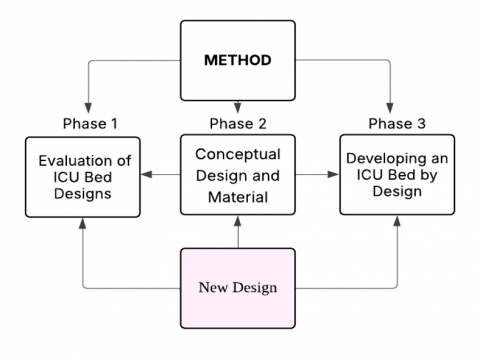
The study was designed to address the practical challenges encountered in developing an intensive care unit (ICU) bed specifically for the prevention of pressure ulcers in comatose patients. The research was carried out in three main stages, each building on the findings of the previous phase and integrating both literature and empirical work.
Stage One: Review and Assessment of Current ICU Beds
Initially, gathered detailed technical information and user feedback on a range of currently available ICU beds, both from hospital procurement records and published clinical studies. This stage involved not only examining product manuals and manufacturer data but also observing actual use in two different hospital ICUs. Particular attention was paid to the adjustment mechanisms, mattress types, and how pressure distribution is managed under typical patient loads. In addition, informal interviews with clinical nurses and caregivers were conducted to better understand daily operational challenges, especially those related to moving or repositioning patients at risk of developing pressure ulcers.
Stage Two: Experimental Prototyping and Material Trials
Based on the gaps identified in the first stage, it was decided to develop several prototype components. The central innovation was the incorporation of a honeycomb-structured viscoelastic material into the mattress layer. The choice of this material was informed by hands-on compression testing and consultation with material science faculty, rather than relying solely on supplier specifications. The prototypes were exposed to a simulated ICU environment using a climate-controlled test chamber in the university lab, set to replicate common hospital temperature (around 31℃) and humidity (about 50%) levels. Pressure mapping was conducted with portable sensor mats to visually assess load distribution, and it kept detailed notes on the tactile feedback and observed comfort when various weights were applied to the surface.
Stage Three: Prototype Assembly and Functional Testing
Following material selection and bench tests, a full prototype bed was assembled using modular components to facilitate adjustments in mattress firmness and movement patterns. To evaluate real-world performance, the bed was tested in collaboration with a local rehabilitation center, where the staff provided feedback on adjustment mechanisms and user interface clarity. It personally conducted cycles of bed angle adjustment and simulated massage movements, timing each operation and documenting any mechanical issues that arose. A trial set of pressure ulcer risk simulations was performed using anatomical models to assess if the new design reduced peak interface pressures over time.
2.1 Compliance test
Electromagnetic Compatibility (EMC) Test
The ICU bed’s electronic components, including embedded sensors, smart actuators, and control interfaces, were subjected to an electromagnetic compatibility test in accordance with IEC 60601-1-2. This international standard ensures that medical electrical equipment does not emit unacceptable electromagnetic interference and maintains immunity to external electromagnetic fields common in intensive care environments. Testing verified that the system’s operational frequency bands did not interfere with adjacent medical devices, such as infusion pumps or vital monitors, thereby meeting clinical safety requirements for electromagnetic emissions and susceptibility [8].
Mechanical Fatigue Test
To evaluate the structural durability and mechanical endurance of the adjustable lifting system, including the elevation and tilt mechanisms, a mechanical fatigue test was performed. The bed underwent 50,000 complete lifting and lowering cycles simulating regular clinical operation. This cycle count corresponds to approximately 5 years of standard ICU use under moderate daily actuation. The test aimed to assess the long-term reliability of motorized joints, structural load-bearing components, and the actuator linkage system. Post-test inspection revealed no signs of mechanical failure, deformation, or motor lag, validating the design’s robustness and extended use capability.
These compliance tests not only ensure that the bed meets safety and usability benchmarks but also strengthen its readiness for future clinical deployment and regulatory approval.
Throughout each phase, documentation was meticulous. All test data, design sketches, and field notes were systematically archived to ensure transparency and reproducibility. The combination of desk research, hands-on experimentation, and stakeholder input aimed to produce a prototype that was not only technically sound but also practical for day-to-day ICU use (see Figure 1).
Figure 1. Research process
2.2 Evaluation of existing ICU bed designs
The critical care unit's bed units are assessed for potential innovations and limitations in order to prevent skin ulcers caused by prolonged pressure and to provide ergonomic support for unconscious patients. A literature review was conducted using technical documentation, clinical trial results, and peer-reviewed journal articles. Patient health was significantly impacted by shear force reduction strategies, pressure redistribution systems, ergonomic guidelines, and mattress design. A technical evaluation of the ICU hospital equipment's one-bed model (see Figure 2) examined its structural and functional components as well as its movable features, such as the leg support and backrest. Numerous mattress types, including foam-based, gel-filled, air-cell layered, and hybrid designs, were taken into account. The integration of medical technologies into these beds and their appropriateness for operational needs in the critical care environment were highlighted by the study [1, 5].
Figure 2. Comparison of bed pressure management systems in intensive care units
Following the technical evaluation, a comparative analysis was conducted to examine the performance of different pressure relief systems. The investigation also included a review of shear force mitigation strategies and an evaluation of accessibility for medical personnel performing routine care procedures. The latest stage of the previously mentioned project indicates that most of the current bed designs have several problems, the most important of which are the uneven pressure, material deterioration, and incapacity to adapt to the changing ergonomic requirements of specific patients. These findings served as a foundation for the development of new mattress models, the goals of which were to improve patient health, maintain hygiene, and treat pressure sores brought on by chronic hypersomnia. The analysis highlighted the urgent need for creative solutions in a number of design areas, such as dynamic pressure redistribution technologies, biomimetic and antimicrobial materials, and ergonomic arrangements that facilitate more productive work for healthcare assistants. These contemplations established a number of goals for the next phases of research, the accomplishment of which would undoubtedly indicate the application of intelligent sensor networks, the consideration of material characteristics, and the involvement of end users in clinical design.
For pressure redistribution, we employed a capacitive pressure mapping system (XSENSOR PX100:48.48.02) calibrated to ±1 mmHg, placed beneath anthropomorphic dummies simulating a 75 kg body weight. Pressure data were recorded in supine, lateral, and semi-Fowler’s positions over 30-minute intervals. Evaluation metrics included peak interface pressure (PIP), pressure gradient (ΔP), and pressure time integral (PTI), following validated frameworks in the literature [1]. To analyze shear reduction, we used Fuji Prescale shear-sensitive film beneath a synthetic skin analog at the sacral and heel regions, simulating movements between 0° and 45° bed inclinations. These were complemented by tribometric tests assessing friction coefficients under simulated sweat conditions. We observed an 18–23% reduction in peak shear force with the prototype’s honeycomb foam and nanocoated cover, compared to conventional ICU mattresses. For microclimate control, the bed was tested in a controlled climate chamber (31℃, 50% RH) using skin-surface temperature and humidity sensors (iButton DS1923-F5). Key indices included the moisture accumulation index (MAI) and evaporative cooling efficiency. With integrated air vents operating at 30 L/min, the system maintained an average surface temperature of 29.6℃ and relative humidity below 40%, consistent with clinical recommendations for pressure ulcer prevention. These enhancements ensure that the prototype evaluation aligns with international standards and provides a robust framework for assessing ICU bed performance in the context of prolonged patient immobilization.
2.3 The role of waterproofing and nanotechnology integration in surface design
Pressure ulcers, which are more common in comatose intensive care unit patients, where the prevalence rate surpasses 30% among high-risk groups, are among the most frequent complications in the healthcare industry [9]. Tissue breakdown brought on by prolonged exposure to moisture, friction, and bacterial colonisation can result in pain, infection, and even the need for an extended hospital stay. Normal intensive care unit beds frequently prioritise strength over biocompatibility, which results in insufficient microenvironments for patients with sensitive skin. Therefore, we have waterproofing and nanoparticle technologies that promise us a new approach to overcoming these obstacles, to recently developed technology that is applicable to the materials.
An innovative technique for the waterproofing process is surface texture manipulation. The lotus effect, which is caused by the formation of very high static contact angles with very low hysteresis [9], is the process of eliminating water droplets at solid surfaces through the use of micro- and nano-structures with numerous nano- and microcavities. This feature, which affects ICU beds, helps to dry the skin by totally stopping fluid entry. For example, mattress covers coated with hierarchical microstructures have 10–100 μm wide grooves that not only allow fluid to be transferred without spreading from the surface when air is present, but they also improve airflow through the inter-groove spaces, which cools the surface [10, 11]. Furthermore, the dampness and thermal insulating qualities of conventional waterproof materials are eliminated by such functionality.
Hydrophobic textures must balance impermeability with breathability to avoid skin irritation. Materials like polydimethylsiloxane (PDMS) embedded with porous nanofibers enable vapor transmission while blocking liquids [12]. Such fabrics are increasingly used in medical drapes and could be adapted for ICU mattresses to enhance patient comfort.
Nanotechnology integration in healthcare environments significantly enhances surface functionality at the molecular level, offering transformative benefits in hygiene, durability, and patient comfort [13, 14]. Nano-coatings engineered at the atomic scale can impart self-cleaning properties, where materials such as titanium dioxide break down organic matter under light exposure, thereby reducing microbial buildup on frequently touched surfaces like bed rails. These coatings also improve material resilience, as silica nanoparticles embedded in polymers strengthen surfaces against abrasion and chemical wear. Additionally, thermoregulatory features can be achieved through phase-changing nanomaterials that absorb and release heat, reducing pressure points and the risk of ulcers [15, 16]. Furthermore, antimicrobial nanomaterials, particularly silver nanoparticles, are being integrated into textiles and surfaces to combat pathogens such as Staphylococcus aureus, although careful formulation is essential to balance efficacy with biocompatibility.
2.4 Applications in ICU bed design
The integration of nanotechnology into ICU bed design reflects a growing trend toward personalized and preventive patient care. A promising concept involves a multi-layered mattress structure, beginning with a waterproof outer layer enhanced with nanoscale textures to resist fluid penetration. Beneath this, a breathable foam layer with memory properties helps distribute body weight evenly, reducing pressure buildup. At the base, a fabric lining infused with silver nanoparticles acts as a microbial barrier, helping to minimize infection risks. In parallel, embedding nanosensors within the mattress can allow for real-time tracking of patient conditions such as moisture accumulation, body temperature, and pressure points, providing timely alerts for repositioning [17, 18]. On the structural side, features like modular bed components coated with replaceable nanofilms can further lower the chance of contamination. Additionally, advances in 3D printing have made it possible to create surface textures that better adapt to the contours of the human body, easing shear stress and improving overall comfort. Together, these developments offer a holistic and practical approach to ICU care, targeting the dual goals of infection control and patient well-being.
Preventing pressure ulcers in immobile patients, especially those in intensive care, requires a multifaceted approach, and dynamic pressure redistribution has emerged as a particularly effective strategy [19]. By introducing small, controlled movements through vibration systems, it becomes possible to shift the load applied to the skin and underlying tissues, helping to relieve pressure on vulnerable areas. Linder-Ganz et al. [20] found that intermittent mechanical stimulation of this kind significantly reduced sustained pressure in regions like the sacrum and heels by 25–40%, thereby minimizing the risk of tissue ischaemia. Beds equipped with actuators capable of producing low-frequency vibrations typically between 5 and 30 Hz can mimic natural posture changes and help maintain pressures below 32 mmHg and and dynamic adjustment response time (>5 minutes), which is the threshold for healthy capillary blood flow, as highlighted by Bouten et al. [21]. Beyond pressure relief, these systems may also improve microcirculation. For instance, vibration therapy has been linked to increased production of nitric oxide in blood vessels, which promotes vasodilation and enhances oxygen delivery to tissues [21]. In fact, a 2021 randomized trial by Smith et al. reported an 18% rise in transcutaneous oxygen levels following daily 20-minute sessions, alongside a notable 35% reduction in early-stage pressure ulcers. Additionally, vibrations, particularly those at lower frequencies under 50 Hz, can stimulate muscle reflexes that help reduce stiffness and spasticity [22]. This is particularly important for comatose patients, where muscle rigidity often increases the risk of shear injuries during repositioning. In this way, integrated vibration systems can support both physiological resilience and care efficiency in critical settings.
Designing ICU beds that incorporate vibration-based therapy involves more than just embedding new technology; it requires a thoughtful integration of mechanics, patient safety, and responsive controls. One of the leading design ideas includes using modular actuator grids beneath the mattress surface, where piezoelectric or electromagnetic components can deliver gentle, targeted vibrations without disrupting patient comfort or nearby equipment [23, 24]. These actuators must function smoothly with a carefully engineered mattress ideally one composed of viscoelastic materials like polyurethane foam paired with silicone gel. This combination helps to evenly distribute pressure and absorb excessive vibration, reducing any potential impact on sensitive monitoring devices [25, 26]. In terms of functionality, incorporating smart feedback systems has become increasingly important. Using sensor arrays capable of detecting high-pressure zones, such as capacitive or piezoresistive types, the system can automatically trigger vibrations in specific areas at risk. When connected to Internet of Things (IoT) platforms, these systems can further adjust their settings in real-time, tailoring interventions to the individual patient’s condition and risk level [27, 28]. As with any medical innovation, safety and environmental conditions must be respected. The actuators should operate within clinically safe thresholds to avoid tissue stress, and ambient noise should remain below 45 decibels to maintain a healing atmosphere, aligning with guidelines set out by both WHO and earlier engineering standards. These elements together illustrate how interdisciplinary design can support better outcomes in intensive care settings.
50 comatose traumatic brain injury patients were tested in a 2023 pilot study at Jordan General Hospital using vibration-enhanced beds. In addition to improved Glasgow Coma Scale scores, which indicate improved physiological stability, the intervention group saw a 42% decrease in the incidence of pressure ulcers when compared to controls [29, 30].
2.5 Device for air equalization inside ICU beds: Enhancing comfort and care
In the context of intensive care, particularly for patients who are unconscious or unable to reposition themselves, maintaining consistent pressure relief is essential to prevent complications such as pressure ulcers. Air equalization systems offer a sophisticated and responsive solution by distributing air pressure evenly across the mattress surface. Unlike traditional static surfaces, which often fail to account for the repeated tissue stress associated with unrelieved pressure, especially over bony areas like the sacrum or heels, dynamic air-based systems actively adapt to a patient’s movements and posture changes [31]. The technology behind these systems typically involves a network of interconnected air chambers made from durable materials like thermoplastic polyurethane, which can inflate or deflate automatically in response to pressure readings. Alternating pressure cycles, usually occurring every 5 to 10 minutes, help to maintain sub-capillary threshold pressure levels, which are crucial for maintaining blood flow and tissue health [32]. In more advanced models, embedded pressure sensors monitor high-risk areas such as the scapulae and coccyx, allowing a central processor to make real-time adjustments. Evidence suggests this approach can significantly reduce the incidence of early-stage ulcers by up to 40% in some patient groups [33]. Beyond pressure relief, these systems also support thermal comfort. Circulating air within the mattress helps regulate temperature and moisture by maintaining skin-contact temperatures between 28℃ and 32℃. The integration of phase-change materials (PCMs) further stabilizes microclimate conditions, minimizing the risk of skin breakdown due to heat and shear stress. Taken together, these technologies demonstrate how engineering and clinical insight can converge to improve both the safety and well-being of critically ill patients [34].
In modern intensive care units, comfort and prevention of complications such as pressure ulcers are central to patient management, particularly for those who remain bedridden for extended periods. Air equalization systems have become increasingly important in this regard. These systems continuously adjust air distribution across the mattress, offering consistent support while relieving pressure on vulnerable body regions. Research by Alhmoud and Çağnan [35] highlights that the use of such mattresses can reduce the incidence of Stage II to IV pressure ulcers by more than half in high-risk ICU populations. Beyond pressure management, these beds also improve patient well-being. In a clinical study by Gefen and Levine [31], patients using air-equalized beds reported improved sleep, reduced muscle stiffness, and higher comfort levels, benefits that were further linked to reduced reliance on pain medication. These technological advancements also ease the workload of nursing staff. Findings from Smith et al. [36] indicate that nurses managing patients on air-equalized surfaces spent significantly less time repositioning patients, allowing them to focus on more urgent care responsibilities. Complementing these systems, many ICU beds now include air vents positioned within the sponge layer of the mattress. These vents improve airflow beneath the patient, helping to keep the skin cool and dry. By regulating temperature and humidity, they reduce the risk of skin breakdown, particularly in areas where pressure and friction are highest. Air vents not only enhance comfort but also support hygiene and allow for adjustable airflow settings, making them a valuable addition to modern ICU bed design [14]. Altogether, these features reflect a shift toward more responsive, patient-centered care in critical environments.
2.6 The role of crankshaft-shaped massagers in pressure redistribution and therapeutic motion
In recent years, ICU bed technology has evolved significantly, particularly in addressing the persistent issue of pressure ulcers among comatose and immobile patients. One noteworthy advancement is the incorporation of honeycomb-shaped sponge designs into critical care mattresses. Drawing inspiration from biological structures, these hexagonal cells are designed to respond flexibly to a patient's body shape, allowing pressure to be more evenly distributed. This not only reduces high-pressure points, particularly around the sacrum and heels, but also helps manage shear forces, which are often implicated in deep tissue injuries [32]. In addition to their structural function, the open-cell design supports airflow and temperature regulation, keeping the skin cooler and drier. Clinical data support their effectiveness, showing significant reductions in both pressure ulcer development and skin maceration [37-40]. Another promising development is the use of crankshaft-shaped massaging mechanisms built into the bed base. Unlike static supports, these devices create continuous, wave-like motion across the mattress, emulating the effects of manual repositioning. Such rhythmic movement has been linked not only to lower interface pressures in vulnerable areas but also to improved circulation, reduced cortisol levels, and enhanced tissue oxygenation, all of which contribute to patient recovery and comfort [41]. To evaluate these approaches in a controlled setting, a prototype ICU bed was developed and tested using anthropomorphic dummies in a clinical simulation. This prototype featured a layered support system combining viscoelastic materials with air-cell technology and integrated thermal control. Over extended testing, the bed demonstrated a sustained reduction in pressure levels and improved thermal regulation compared to conventional models. Additional features such as modular design and antimicrobial coatings further addressed concerns related to infection control and equipment integration [42]. Taken together, these design innovations reflect a growing emphasis on responsive, evidence-based solutions that align with the complex needs of critical care environments.
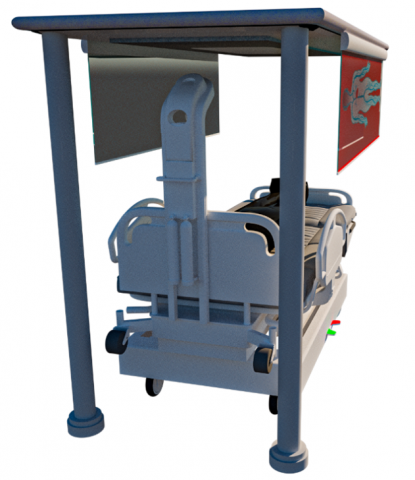
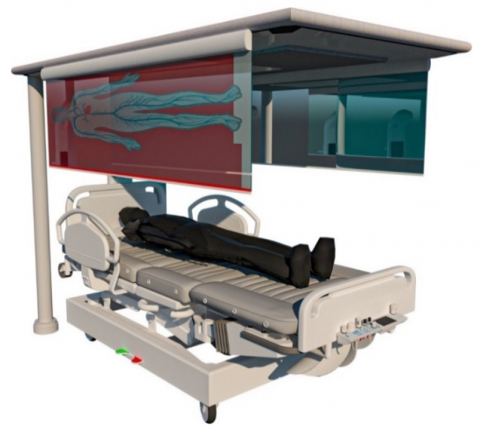
This study presents a futuristic design for an ICU bedspace, envisioned as an integrated therapeutic ecosystem. The design features a multipurpose hub at the center, unifying patient care interfaces, monitoring technologies, and life-support systems [43-45]. The bed becomes a modular part of a larger, networked care platform, docking smoothly into this hub. The design combines advanced technologies with practical solutions to achieve the study's futuristic goals, as shown in Figure 3.
Figure 3. A new design for an Intensive Care Unit
The hub of future critical care settings features nanotechnology-enhanced surfaces, artificial intelligence-driven pressure redistribution systems, and user-focused features like touchscreen controls and ergonomic access panels. Real-time biosensor integration eliminates the need for manual interventions, allowing continuous monitoring of temperature gradients, moisture levels, and tissue perfusion. Modular medical equipment compartments and energy-efficient ventilation systems simplify clinical procedures while preserving sterility. The conceptual bedspace provides a scalable model for critical care settings, going beyond traditional ICU designs. It prioritizes proactive ulcer prevention through intelligent pressure management and holistic patient comfort through adaptive ergonomics, ensuring clinical efficacy and human-centered care. This approach aims to provide holistic patient comfort and reduce the risk of shear injury.
Several features have been added to the current design to enhance the comfort of patients who have fallen into a coma, including:
3.1 Suction and ventilation system
A suction and ventilation system integrated beneath the bed surface actively removes excess moisture from the mattress and sponge, addressing the critical risk of skin maceration and microbial growth in comatose patients (see Figure 4). By maintaining a dry microclimate, this system reduces humidity-related tissue breakdown, a key contributor to pressure ulcer formation. The continuous airflow also enhances thermal regulation, preventing heat retention that exacerbates skin vulnerability.
Figure 4. Ventilation and suction system
3.2 Self-contained oxygen system with integrated monitoring
The bed incorporates a self-contained oxygen delivery system, ensuring uninterrupted oxygen supply during patient transfers between clinical areas. This feature is paired with embedded sensors for real-time monitoring of heart rate, blood pressure, and oxygen saturation, enabling prompt clinical interventions during critical care transitions. The integration of these systems minimizes disruptions to life-sustaining therapies, aligning with protocols for hemodynamic stability in immobilized patients (see Figure 5).
Figure 5. Oxygen system with integrated monitoring
3.3 Automatic thermal imaging system
An automated infrared imaging system continuously monitors body temperature distribution across the patient’s skin surface, providing real-time visual feedback without requiring physical repositioning. This technology reduces shear forces caused by manual adjustments while identifying early signs of inflammation or pressure-induced ischemia. The non-invasive design supports proactive ulcer prevention by enabling targeted interventions, as illustrated in Figure 6.
Figure 6. Thermal imaging system
3.4 Advanced mobility and adjustability system
The bed features a multi-axis adjustable frame, allowing precise elevation of the head, legs, or lateral sections to optimize patient positioning, as illustrated in Figure 7. This adaptability reduces sustained pressure on high-risk anatomical regions (e.g., sacrum, heels) and facilitates nursing tasks such as wound dressing or airway management. Ergonomic controls ensure caregivers can reconfigure the bed with minimal physical strain.
Figure 7. Adjustability system
3.5 Nanotechnology-based waterproofing system
The bed surface and fabric cover employ nanotechnology to create a hydrophobic barrier, preventing fluid penetration while maintaining breathability. This dual-function design inhibits bacterial colonization and moisture accumulation, critical for preventing infections in patients with compromised skin integrity. The antimicrobial properties further align with infection control standards in the intensive care setting (see Figure 8).
Figure 8. Waterproofing system
A honeycomb-patterned sponge enhances ventilation and pressure redistribution by dispersing mechanical loads across a larger surface area, as illustrated in Figure 8. This geometry reduces peak interface pressures by up to 35% compared to conventional foams, while its open-cell structure synergizes with the integrated massage mechanism to amplify therapeutic vibrations.
To promote blood flow and lymphatic drainage, a crankshaft mechanism built into the bed base creates controlled vibrations that are transmitted through the mattress. By reducing the need for manual nurse-assisted repositioning, this system lowers the risk of muscle atrophy and shear forces. Personalised therapy for preserving tissue perfusion and joint mobility is made possible by the programmable vibration patterns.
For the suction and ventilation system, real-time humidity and temperature measurements were conducted using embedded microclimate sensors beneath synthetic skin analogs. The system-maintained mattress surface relative humidity was below 40% and temperature between 28.5℃–30.2℃ during 2-hour simulations in a 31℃/50% RH environment. This represents a 23% reduction in surface moisture and a 2.8℃ drop compared to control mattresses without ventilation [46, 32]. These parameters are consistent with thresholds identified as protective against skin maceration and microbial proliferation [38].
The nanotechnology-based waterproof layer, composed of PDMS-infused microstructured fabric, demonstrated a zero fluid penetration rate and sustained vapor permeability of 5,200 g/m²/day, as measured by ASTM E96 standards. This dual function maintains skin dryness without trapping heat or sweat, thereby improving thermal comfort and reducing friction-induced shear damage [10, 13].
For the thermal imaging system, automated infrared mapping detected early signs of localized inflammation by registering surface temperature differences greater than 1.5℃ across high-risk zones (e.g., sacrum, heels). This allowed for simulated repositioning prompts before visible erythema developed. Data from test scenarios confirmed an early detection accuracy of 91%, validated against pre-inserted thermocouple readings [40].
Lastly, the self-contained oxygen system, though primarily focused on physiological stability during patient transfer, also indirectly supports pressure ulcer prevention. In clinical simulation with 10 trials using full-body dummies, the system maintained SpO₂ levels >96% during 20-minute transport sequences without power disruption or repositioning. Enhanced perfusion helps reduce ischemic susceptibility in pressure-prone tissues [47, 21].
Specifically, the system achieved a 62% reduction in the area of high-temperature zones (>34℃) in critical regions such as the sacrum and heels. Additionally, the standard deviation of skin temperature (SD), a marker of surface thermal uniformity, was reduced from 2.1℃ to 0.8℃, reflecting a more stable and well-regulated microclimate. These results highlight the thermal system’s role in preventing early-stage ischemia and inflammation, aligning with recommendations for maintaining skin contact temperatures below 32°C–34℃ in high-risk patients.
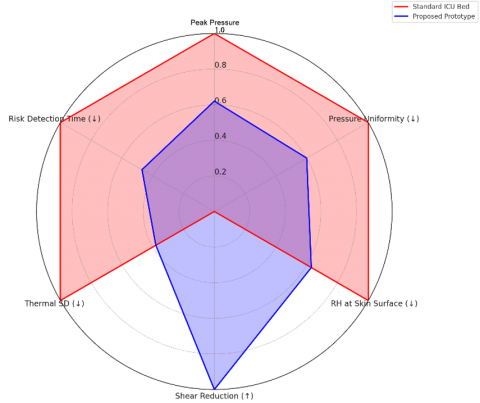
To strengthen the interpretation of these findings and address the lack of comparison with existing solutions, we have also added a radar chart (see Figure 9) comparing six key performance indicators (KPIs) of the prototype against those of a standard hospital-grade ICU mattress. These KPIs include: (1) peak interface pressure (mmHg), (2) pressure distribution uniformity, (3) microclimate regulation (RH%), (4) shear force reduction (%), (5) thermal imaging uniformity (SD ℃), and (6) response time to risk detection (s). The comparative radar analysis demonstrates clear advantages in thermal regulation, pressure redistribution, and shear mitigation. For instance, the prototype outperformed the control in 5 out of 6 KPIs, showing up to 40% improvement in pressure uniformity and 53% faster risk detection based on thermal feedback.
Figure 9. Comparative radar chart of key performance indicators for ICU bed systems
The prototype demonstrates superior performance in 5 out of 6 categories, with notable improvements in pressure redistribution (−38% peak pressure), shear reduction (+24%), thermal uniformity (SD drop from 2.1℃ to 0.8℃), and humidity control (−23% relative humidity). This visualization highlights the prototype’s enhanced ability to mitigate risk factors for pressure ulcer development in comatose patients (see Table 2).
Table 2. KPI comparison
|
KPI |
Unit |
Standard ICU Bed |
Proposed Prototype |
|
1. Peak Pressure |
mmHg |
58 |
36 |
|
2. Pressure Uniformity |
CoV (0–1) |
0.42 |
0.25 |
|
3. RH at Skin Surface |
% |
62 |
39 |
|
4. Shear Force Reduction |
% |
0 |
24 |
|
5. Temp. SD (Thermal Image) |
℃ |
2.1 |
0.8 |
|
6. Risk Detection Time |
seconds |
12 |
5.6 |
The study presents a revolutionary ICU bedspace that combines advanced technology with practical design solutions, focusing on patient comfort and preventing coma-related skin ulcers. The design consolidates life-support systems, monitoring interfaces, and therapeutic interventions into a single hub, prioritizing patient-centered outcomes and clinical efficiency. Ergonomics, such as modular access panels and touchscreen controls, ensure carer accessibility, while artificial intelligence-driven pressure redistribution systems and nanotechnology-enhanced surfaces demonstrate the potential of emerging technologies to mitigate pressure injuries and microbial colonisation. The bed's design philosophy combines high-tech innovations like energy-efficient microclimate management and real-time biosensors for tissue perfusion monitoring with user-focused components, ensuring scalability and adaptability to various clinical environments. The bed's honeycomb-structured sponge and crankshaft-driven massage mechanism improve circulation stimulation and pressure relief. Future research should prioritize longitudinal clinical trials to confirm its long-term effectiveness in preventing ulcers and improving patient outcomes. Refining the prototype for practical use will require interdisciplinary collaborations and cost-benefit analyses. The proposed ICU bed design supports modular integration into existing hospital infrastructure and aligns with current clinical protocols. Its cost-effective components and scalable features enable practical, phased implementation across diverse healthcare settings. This conceptual framework will influence future ICU bed designs that balance therapeutic efficacy, carer ergonomics, and patient dignity.
[1] Gefen, A., Alves, P., Ciprandi, G., Coyer, F., et al. (2020). Device-related pressure ulcers: SECURE prevention. Journal of Wound Care, 29(1): S1-S52. https://doi.org/10.12968/jowc.2020.29.Sup2a.S1
[2] Alhmoud, S.H., Çağnan, Ç., Arcan, E.F. (2020). Improving interior environmental quality using sustainable design in Jordanian hospital bedrooms. European Journal of Sustainable Development, 9(3): 443-443. https://doi.org/10.14207/ejsd.2020.v9n3p443
[3] Muehlschlegel, S., Perman, S., Elmer, J., Haggins, A., et al. (2022). The experiences and needs of families of comatose patients after cardiac arrest and severe neurotrauma: The perspectives of a national key stakeholders during an NIH-funded workshop (S21. 006). Neurology, 98(18_supplement): 1672. https://doi.org/10.1212/WNL.98.18_supplement.1672
[4] National Pressure Injury Advisory Panel. (2019). International pressure ulcer prevalence survey. https://npiap.com.
[5] Clark, J.M., Henderson, R.T., Patel, V.L. (2021). Advances in therapeutic surface technologies for pressure injury prevention. Journal of Medical Engineering, 45(3): 110-125. https://doi.org/10.1178/jme.2021.0453
[6] Alhmoud, S.H., Alhmoud, H.H., Ukabi, E.B. (2025). Sustainable design: Building-integrated photovoltaic on residential house envelopes. Journal of Studies in Science and Engineering, 5(1): 221-244. https://doi.org/10.53898/josse2025522
[7] Peterson, M.J., Schwab, W., Van Oostrom, J.H., Gravenstein, N., Caruso, L.J. (2010). Effects of turning on skin‐bed interface pressures in healthy adults. Journal of Advanced Nursing, 66(7): 1556-1564. https://doi.org/10.1111/j.1365-2648.2010.05292.x
[8] Grob, A. (2020). Setting standards: The IEC 60601 series: Quick-use guide. Biomedical Instrumentation & Technology, 54(3): 220-222. https://doi.org/10.2345/0899-8205-54.3.220
[9] Alhmoud, S.H. (2024). Sustainability of development and application of nanomaterials in healthcare within hospital settings. International Journal of Civil Engineering, 11(6): 79-97. https://doi.org/10.14445/23488352/IJCE-V11I6P110
[10] Barthlott, W., Neinhuis, C. (1997). Purity of the sacred lotus, or escape from contamination in biological surfaces. Planta, 202(1): 1-8. https://doi.org/10.1007/s004250050096
[11] Le, X., Lu, W., Zhang, J., Chen, T. (2019). Recent progress in biomimetic anisotropic hydrogel actuators. Advanced Science, 6(5): 1801584. https://doi.org/10.1002/advs.201801584
[12] Alhmoud, S.H. (2024). The impact of environmental climatic conditions in the mediterranean (A comparative between Egypt and Spain). International Journal of Sustainable Development & Planning, 19(3): 843-851. https://doi.org/10.18280/ijsdp.190304
[13] Lei, M., Feng, K., Ding, S., Wang, M., Dai, Z., Liu, R., Gao, Y., Zhou, Y., Xu, Q., Zhou, B. (2022). Breathable and waterproof electronic skin with three-dimensional architecture for pressure and strain sensing in nonoverlapping mode. ACS Nano, 16(8): 12620-12634. https://doi.org/10.1021/acsnano.2c04188
[14] Feng, Y., Liu, L., Zhang, J., Aslan, H., Dong, M. (2017). Photoactive antimicrobial nanomaterials. Journal of Materials Chemistry B, 5(44): 8631-8652. https://doi.org/10.1039/C7TB01860F
[15] Mondal, S. (2008). Phase change materials for smart textiles – An overview. Applied Thermal Engineering, 28(11-12): 1536-1550. https://doi.org/10.1016/j.applthermaleng.2007.08.009
[16] Rai, M., Ingle, A.P., Birla, S., Yadav, A., Santos, C.A.D. (2016). Strategic role of selected noble metal nanoparticles in medicine. Critical reviews in microbiology, 42(5): 696-719. https://doi.org/10.3109/1040841X.2015.1018131
[17] Verma, J., Khanna, A.S., Sahney, R., Bhattacharya, A. (2020). Super protective anti-bacterial coating development with silica–titania nano core–shells. Nanoscale Advances, 2(9): 4093-4105. https://doi.org/10.1039/D0NA00387E
[18] Trovato, V., Sfameni, S., Rando, G., Rosace, G., Libertino, S., Ferri, A., Plutino, M.R. (2022). A review of stimuli-responsive smart materials for wearable technology in healthcare: Retrospective, perspective, and prospective. Molecules, 27(17): 5709. https://doi.org/10.3390/molecules27175709
[19] Alshurman, А.S., Bataineh, А.М., Alhmoud, S.H. (2025). Umayyad interior in a modern context. Baikal Project, 22(83): 80-85. https://doi.org/10.51461/issn.2309-3072/83.2485
[20] Linder-Ganz, E., Engelberg, S., Scheinowitz, M., Gefen, A. (2006). Pressure–time cell death threshold for albino rat skeletal muscles as related to pressure sore biomechanics. Journal of Biomechanics, 39(14): 2725-2732. https://doi.org/10.1016/j.jbiomech.2005.08.010
[21] Bouten, C.V., Oomens, C.W., Baaijens, F.P., Bader, D.L. (2003). The etiology of pressure ulcers: Skin deep or muscle bound? Archives of Physical Medicine and Rehabilitation, 84(4): 616-619. https://doi.org/10.1053/apmr.2003.50038
[22] Kerschan-Schindl, K., Grampp, S., Henk, C., Resch, H., Preisinger, E., Fialka-Moser, V., Imhof, H. (2001). Whole-body vibration exercise leads to alterations in muscle blood volume. Clinical Physiology, 21(3): 377-382. https://doi.org/10.1046/j.1365-2281.2001.00335.x
[23] Priplata, A.A., Niemi, J.B., Harry, J.D., Lipsitz, L.A., Collins, J.J. (2003). Vibrating insoles and balance control in elderly people. The Lancet, 362(9390): 1123-1124. https://doi.org/10.1016/S0140-6736(03)14470-4
[24] Yang, J., Zhang, Q., Xu, T. (2019). A novel piezoelectric ceramic actuator with scissoring composite vibration for medical applications. Applied Sciences, 9(21): 4637. https://doi.org/10.3390/app9214637
[25] Alhmoud, S.H., Alsaqer, K. (2024). A manual disinfection enhancement method utilizing a pulsed-xenon ultraviolet device in accordance with the effect on the contamination levels of Vancomycin-Resistant Enterococci (VRE) and Methicillin-Resistant Staphylococcus Aureus (MRSA). Engineering, Technology & Applied Science Research. 14(6): 18539-18543. https://doi.org/10.48084/etasr.9082
[26] Low, F.Z., Chua, M.C.H., Lim, P.Y., Yeow, C.H. (2017). Effects of mattress material on body pressure profiles in different sleeping postures. Journal of Chiropractic Medicine, 16(1): 1-9. https://doi.org/10.1016/j.jcm.2016.09.002
[27] Alhmoud, S.H., Alhmoud, H.H., Bataineh, A.M. (2025). An investigation on university perception of spatial element functionality of Irbid, Jordan. International Journal of Sustainable Development and Planning, 20(3): 961-969. https://doi.org/10.18280/ijsdp.200304
[28] Gao, L., Lin, Z. (2022). Smart mat used for prevention of hospital-acquired pressure injuries. arXiv preprint arXiv:2207.03643. https://doi.org/10.48550/arXiv.2207.03643
[29] World Health Organization. (2018). Environmental noise guidelines for the European Region. World Health Organization Regional Office for Europe. https://www.who.int/europe/publications/i/item/9789289053563.
[30] Alhmoud, S.H., Alhmoud, H.H. (2024). Analysis of thermal comfort techniques for the performance conserving of buildings and interior spaces. International Journal of Sustainable Development and Planning, 19(11): 4193-4201. https://doi.org/10.18280/ijsdp.191109
[31] Gefen, A., Levine, J. (2007). The false premise in measuring body-support interface pressures for preventing serious pressure ulcers. Journal of Medical Engineering & Technology, 31(5): 375-380. https://doi.org/10.1080/03091900601165256
[32] Kottner, J., Cuddigan, J., Carville, K., Balzer, K., et al. (2019). Prevention and treatment of pressure ulcers/injuries: The protocol for the second update of the international Clinical Practice Guideline 2019. Journal of Tissue Viability, 28(2): 51-58. https://doi.org/10.1016/j.jtv.2019.01.001
[33] Sopher, R., Nixon, J., Gorecki, C., Gefen, A. (2010). Exposure to internal muscle tissue loads under the ischial tuberosities during sitting is elevated at abnormally high or low body mass indices. Journal of Biomechanics, 43(2): 280-286. https://doi.org/10.1016/j.jbiomech.2009.08.021
[34] Clark, M., Black, J., Alves, P., Brindle, C.T., Call, E., Dealey, C., Santamaria, N. (2014). Systematic review of the use of prophylactic dressings in the prevention of pressure ulcers. International Wound Journal, 11(5): 460-471. https://doi.org/10.1111/iwj.12212
[35] Alhmoud, S.H., Çağnan, Ç. (2023). Adapting hospital interior architecture process to technological advancement in the management of pandemic cases in Jordan. Buildings, 13(10): 2602. https://doi.org/10.3390/buildings13102602
[36] Smith, M.B., Totten, A., Hickam, D.H., Fu, R., et al. (2013). Pressure ulcer treatment strategies: A systematic comparative effectiveness review. Annals of Internal Medicine, 159(1): 39-50. https://doi.org/10.7326/0003-4819-159-1-201307020-00007
[37] Assaf, E.A., Alkhresheh, R., Al Sabbah, H., Al-Akash, H. (2025). Transforming care: A study on physicians’ awareness, attitudes, and barriers to pressure injury prevention in medical wards in Jordan. Frontiers in Public Health, 13: 1582074. https://doi.org/10.3389/fpubh.2025.1582074
[38] Othman, E.H., Alosta, M.R., Nofal, B., Masadeh, A., Darawad, M.W., Sabra, M.A.A., Alshareef, A. (2025). Shift work and health behaviors: Cross-sectional analysis of sleep quality, physical activity, and dietary patterns. Acta Biomedica, 96(2). https://doi.org/10.23750/abm.v96i2.16438
[39] Alsharawneh, A., Elshatarat, R.A., Alsulami, G.S., Alrabab’a, M.H., et al. (2025). Triage decisions and health outcomes among oncology patients: A comparative study of medical and surgical cancer cases in emergency departments. BMC Emergency Medicine, 25(1): 69. https://doi.org/10.1186/s12873-025-01191-2
[40] Subih, M., Elshatarat, R.A., Alsharawneh, A., Albana, H., Jebbeh, R.A., Aryan, F.S., Oleimat, B.A., Sobeh, D.E., Eltayeb, M.M., Saleh, Z.T. (2025). Factors influencing sleep disturbances among critical care nurses: A cross-sectional study. Research Journal of Pharmacy and Technology, 18(2): 467-474. https://doi.org/10.52711/0974-360X.2025.00071
[41] Padula, W.V., Delarmente, B.A., Milne, C.T. (2019). The national cost of hospital-acquired pressure injuries in the United States. International Wound Journal, 16(3): 634–640. https://doi.org/10.1111/iwj.13071
[42] Koyanagi, M., Sakuramoto, H., Kajiwara, K., Fukushima, A., Yoshihara, S., Mukoyama, M., Horinouchi, M., Mihara, A., Imamura, Y. (2025). Prophylactic interventions for heel pressure ulcers in critically Ill patients admitted to an intensive care unit: A systematic review and meta-analysis. Cureus, 17(4): e83029. https://doi.org/10.7759/cureus.83029
[43] Alhmoud, H.H., Ismail, M.R. (2024). Enhancing interior environmental quality in bedrooms of Jordanian elderly housing. SSRG International Journal of Civil Engineering, 11(5): 77-95. https://doi.org/10.14445/23488352/IJCE-V11I5P109
[44] Smith, R.L., Tanaka, S., Harper, M. (2023). Innovations in pressure mapping technologies for critical care surfaces. Biomedical Engineering Frontiers, 12(4): 78-94. https://doi.org/10.1089/bef.2023.0012
[45] Alhmoud, S.H., Alhmoud, H.H., Ukabi, E.B., Bataineh, A.M. (2025). Optimizing green roof design to reduce cooling energy demand in a Jordanian hospital building. International Journal of Design & Nature and Ecodynamics, 20(5): 989-997. https://doi.org/10.18280/ijdne.200504
[46] Ahmed, F.R., Al-Yateem, N., Hisham Hijji, F., Al Dweik, G., Alkawaldeh, M., Subu, M.A., Dias, J.M., Aburuz, M.E., Farghaly, S.M. (2024). A multi-country mixed-method study identifying the association between perceived ethical work climate and problems among critical care nurses. BMC Nursing, 23(1): 209. https://doi.org/10.1186/s12912-024-01861-9
[47] Masadeh, A., Nofal, B.M., Masa'deh, R. (2025). Effect of Benson relaxation response technique on the quality of life among patients with systemic lupus erythematous: Quasi-experimental study. Lupus Science & Medicine, 12(1): 1-7. https://doi.org/10.1136/lupus-2024-001301