Mohammed S. Hashim Almatwari*![]() | Mohammed Qasim Yahya Malallah A. Al-Atrakji
| Mohammed Qasim Yahya Malallah A. Al-Atrakji![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Acute kidney injury (AKI) is a critical clinical condition characterized by a sudden loss of kidney function. AKI is commonly associated with rhabdomyolysis (RML), which often results from myoglobin release. This leads to oxidative stress, inflammation, endothelial damage, and tubular necrosis. Currently, therapeutic options for AKI are limited, spurring interest in natural compounds with nephroprotective effects. This study investigates the protective effects of Liquiritigenin (LQ), a licorice-derived chiral flavonoid. Due to its simple structure, LQ exhibits good absorption and bioavailability. As a selective estrogen-β agonist, it inhibits cytokine gene expression, exerts substantial scavenging activity against reactive species, restores mitochondrial integrity, promotes antioxidant enzyme production, and downregulates cytokine expression. This study investigates the strong antioxidant and anti-inflammatory properties of LQ in a glycerol (GLY)-induced AKI model. Sixty male albino rabbits were divided into five groups: control, AKI-induced group (induction), vehicle group, and two treatment groups treated with LQ (30 mg/kg and 50 mg/kg, respectively). AKI was induced by a single intramuscular injection of hypertonic glycerol. Biochemical analyses included measurements of serum creatinine, urea, creatine kinase (CK), electrolytes, oxidative stress markers (glutathione peroxidase [GPx1] and malondialdehyde [MDA], and inflammatory cytokines (IL1β, IL6, TNF-α). Kidney tissues were examined histologically to assess structural damage. The GLY-induced AKI group exhibited significantly elevated serum creatinine, urea, CK, proinflammatory cytokines, and MDA, alongside decreased GPx1 levels and substantial histopathological damage. In contrast, the LQ treatment groups, especially at 50 mg/kg, showed significant reductions in serum creatinine, urea, CK levels, and inflammatory cytokines, with a notable improvement in GPx1 and a decrease in MDA levels. Electrolyte imbalances observed in the GLY group were also restored in the LQ-treated groups. Histopathological analysis revealed decreased tubular injury and overall tissue recovery in the LQ-treated groups. LQ demonstrated significant nephroprotective effects in GLY-induced AKI, through the inhibition of oxidative stress-induced tubular injury, downregulation of pro-inflammatory cytokines, and preservation of renal tubular structure. These findings suggest that LQ is a promising therapeutic candidate for managing AKI, particularly in cases associated with RML.
AKI, rhabdomyolysis, liquiritigenin, oxidative stress, myoglobinuria, inflammation
Acute kidney injury (AKI) is a severe clinical condition characterized by an abrupt yet reversible reduction in kidney function within hours to days. It is defined by an increase of at least 0.3 mg/dL in serum creatinine within 48 hours and/or reduced urine output (oliguria) for at least six hours. This situation may be expanded for 7 days or less [1].
Previously, the term “acute renal failure” (ARF) was used to describe this clinical condition before being redefined as AKI [2]. It highly affects hospitalized patients, about 10-15% of total inpatients and 50% of critically ill patients [3]. This syndrome is associated with a high mortality rate. Although various medications have been used to restore normal renal function, their cost places a significant financial burden on patients [4]. It causes up to 1.7 million yearly deaths [5].
AKI is attributed to various reasons, including dehydration, sepsis, medication toxicity, and internal substances, such as hemoglobin in cases of hemolysis and myoglobin (Mb) in cases of RML, which have potential nephrotoxicity for renal tubules, and underlying chronic conditions such as diabetes or hypertension [6]. AKI is a critical health challenge that may progress to chronic kidney disease (CKD), especially in elderly patients and those with comorbidities [7].
RML is one of the main contributors to AKI [8]. It refers to the rapid breakdown of striated muscles and the diffusion of Intracellular contents like CK, lactate dehydrogenase (LDH), Mb, phosphates, and potassium (K+) into the blood circulation [9]. RML is a multifactorial syndrome, including trauma caused by road traffic accidents, nephrotoxic drugs, poisonous materials, extensive muscle workouts, surgical operations, infectious disease, body temperature alteration, epilepsy, and genetic disorders [10]. Biochemically, CK is considered a diagnostic criterion for RML and is highly increased, reaching more than fivefold the upper limit value or >1,000U/L during 2-12 hours and peaking within 24-72 hours following the muscle injury. Serum CK concentration is believed to be a preferable predictor of AKI [11].
The prevalence of AKI caused by RML is considerably high, comprising 15% of all RML cases and accounting for 40% of total AKI cases. It is the leading cause of death among RML patients due to renal injury [12]. Several studies have proposed diverse pathogenic mechanisms for RML-mediated AKI, including (1) vasoconstriction due to hypovolemia and the release of potent vasoconstrictors, (2) Mb-induced oxidative stress and tubular cast formation, and (3) inflammation. A study by Hebert et al. [13] concluded that the release of vast amounts of potentially nephrotoxic substances, specifically Mb and uric acid, contributes to AKI development.
It was reported that extract of the dried rhizomes of licorice is usually used for its life-enhancing attributes, the management of injuries or inflammatory disorders, and detoxification in traditional Chinese medicine, as well as widely used as food supplement products attributed mainly to flavonoids, the main active ingredients of licorice radix [14]. Liquiritigenin (7,4′-dihydroxyflavanone) is a dihydroflavonoid constituent derived from licorice radix, primarily from Glycyrrhiza uralensis [15]. It was approved that LQ has antioxidants, anti-inflammatory, antiproliferation, anti-tumor and antihyperlipidemic effects [16]. Previous studies demonstrated the nephroprotective effects of LQ against cisplatin-mediated AKI through the recovery of mitochondrial damage of renal tubular epithelial cells via attenuating the reactive oxygen species (ROS) generation that mitigates oxidative stress [17]. Moreover, LQ showed kidney protective effects against AKI mediated by intravenously administered folic acid by attenuating ferroptosis induced by iron aggregation [18].
After muscle breakdown, serum Mb is markedly elevated, freely filtered by the glomerulus, reabsorbing and accumulating inside renal tubules, subsequently breaking down and releasing free iron [18, 19]. Mb-ferrous (Fe2+) form, essential for oxygen-carrying, oxidized to ferric iron (Fe3+) by an oxidation reaction causes the liberation of hydroxyl radicals (OH·) (Fenton reaction) inside the tubular cell, Mb- derived Fe+3 tends to be more stable and converts via redox cycle to ferryl Mb (Mb-Fe+4), generating additional reactive metabolite and further precipitating oxidative stress causing peroxidation of the lipid membrane and cellular denaturation [20].
Oyagbemi et al. [21] reported that inflammation plays a pivotal role in the development of AKI associated with RML. Following muscle lysis, the release of toxic materials stimulates the production of proinflammatory mediators such as interleukin-1β (IL1β), interleukin-6 (IL6), and tumor necrosis factor-alpha (TNF-α), leading to intense renal vascular resistance (RVR) and ischemic injury. Mb precipitate in renal tubules activates the complement system, nuclear factor kappa B (NF-κB), Toll-like receptors (TLRs), which trigger cellular immunity, and Phagocytes. Inflammatory mediators like transforming growth factor beta (TGF-β) and TNF-α, stimulated by these signaling pathways, lead to the maintenance of inflammation [21]. Pro-inflammatory mediators like IL1β and IL6 are produced due to various harmful stimulations, such as infections and different forms of inflammation. These are essential in stimulating and progressing inflammatory responses, encouraging the inflammatory acute phase, and promoting injured tissue repair [22]. Mb-derived iron promotes oxidative stress by generating reactive species that injure the tubular cell and stimulate the release of cytokines and chemokines, enhancing the leukocyte adhesion to the epithelial cell and necrosis of renal tubular cells [23].
In this study, we aim to assess the protective effects of the flavonoid LQ against AKI induced by GLY-mediated myoglobinuria in rabbits, exploring the potential antioxidant and anti-inflammatory mechanisms to mitigate renal damage.
2.1 Animals
The study conducted from December 2023 to July 2024, used sixty healthy male albino rabbits; only male rabbits were included, while females were excluded to eliminate potential sex-related physiological variations sourced from the Basra College of Medicine animal facility at Al-Basra University. The rabbits underwent a two-week acclimatization period before experimentation. This research followed the Guide for the Care and Use of Laboratory Animals and was approved by the Animal Ethics Committee of the College of Medicine, Baghdad University. The rabbits, aged 6 months to 1 year and weighing 1-2 kg, were housed under controlled conditions of 25 ± 2℃ temperature, 50 ± 5% humidity, and a 12-hour light/dark cycle. They were kept in five cages, with 12 rabbits per cage, and had free access to water and chewable food.
2.2 Experimental design
The rabbits were randomly divided into five groups of 12 each. After 24 hours of water deprivation, AKI was induced using the method described by Hareedy et al. [24], with minor modifications. A single deep intramuscular (IM) injection of glycerol (50% v/v) at a dose of 8 ml/kg was administered. This dose was selected based on our pilot study, which tested different doses (7, 8, and 10 ml/kg) in five animals per dose. After 24 hours, renal function markers, electrolytes, and CK levels were measured to determine the most efficient glycerol dose for inducing AKI with minimal mortality. The dose was divided equally between both rear limbs and administered on the third day to all groups except the control group, which received normal saline (0.9%). The LQ was dissolved in a vehicle solution composed of dimethyl sulfoxide (DMSO), Tween 80, and distilled water in a ratio of 10:15:75. This vehicle solution was selected based on a previous study, and we conducted a pilot study to examine the solubility of LQ in this solution. To our knowledge, this vehicle solution has been used previously to dissolve licorice active constituents, such as isoliquiritigenin and LQ, without affecting LQ bioavailability. The groups were as follows:
Control Group: Received 5 ml distilled water intraperitoneally (IP) without any GLY treatment.
Induction Group (GLY): On the third day, a single IM injection of 8 ml/kg hypertonic GLY solution was received.
Vehicle Group: Administered the vehicle solution IP for five days, with a GLY injection on the third day.
LQ30 Group: Treated with 30 mg/kg LQ IP for five days and received a GLY injection on the third day.
LQ50 Group: Treated with 50 mg/kg LQ IP for five days and received a GLY injection on the third day.
After 24 hours following the last dose, animals were anesthetized, and blood was collected for biochemical analyses. Kidneys were then harvested for histopathological examination.
2.3 Reagents and materials
Liquiritigenin (purity ≥98%) was purchased from Chengdu Bio Purify Phytochemicals Ltd. Other reagents, including DMSO, Tween 80, and protease inhibitors, were sourced from Med Chem Express. ELISA kits were acquired from ELK Biotechnology Co. Ltd (Wuhan).
2.4 Serum collection and biochemical analysis
Following the last administered dose, all rabbits were fasted for two hours before anesthesia. The euthanasia protocol included 35 mg/kg ketamine, 5 mg/kg xylazine hydrochloride, and 0.1 mg/kg acepromazine maleate [25]. Approximately 3 ml of blood was drawn, allowed to clot for 15 minutes, and centrifuged at 4000 g for 10 minutes. The resulting serum was separated and stored in labeled Eppendorf tubes at -20℃ for later biochemical analyses, including serum urea, creatinine, electrolytes sodium (Na⁺), K⁺, calcium (Ca²⁺), and CK levels as indicators of rhabdomyolysis and AKI.
2.5 Biochemical markers assessment
Renal Function Markers: Serum urea and creatinine levels were measured using specific kits and the Mindray BS-240 clinical biochemistry analyzer, according to the manufacturer’s instructions.
Serum CK levels were assessed to indicate RML using a specific kit, according to the manufacturer’s instructions, with the Mindray BS-240 analyzer.
Serum electrolytes: The sodium, potassium, and calcium concentrations were determined using dedicated kits and the Mindray BS-240 analyzer.
2.6 Kidney tissue collection and preparation
After euthanasia, both kidneys were harvested, rinsed with normal saline to remove excess blood, decapsulated, and cross-sectioned. The left kidneys were preserved in 10% formalin for histopathological evaluation. In contrast, the right kidneys were placed in phosphate-buffered saline (PBS) and stored at -80℃ for later preparation of tissue homogenates for oxidative stress and inflammatory marker analysis.
2.7 Preparation of tissue homogenates and marker analysis
Tissue homogenates were prepared from the right kidneys, which were thawed and washed with ice-cold PBS to remove clots. The tissues were minced into small pieces, weighed, and homogenized in fresh lysis buffer (PBS, pH 7.4) at a 1:9 w/v ratio (e.g., 100 mg of tissue with 900 μl lysis buffer) using a tissue homogenizer. The homogenates were centrifuged at 4℃ at 10,000 g for 5 minutes using a cooling centrifuge. The supernatant was collected, divided into aliquots to prevent repeated freeze-thaw cycles, and stored at ≤ -20℃ until inflammatory and oxidative marker assessments were conducted using ELISA.
2.8 Histopathological examination of kidney tissues
The left kidneys, preserved in formalin, were sectioned into 5-μm slices, stained with hematoxylin and eosin (H&E), and prepared according to Bancroft’s Manual of Histological Techniques [26]. Histopathological changes were observed under a light microscope and evaluated based on the following criteria: interstitial vascular congestion, glomerular atrophy and congestion, interstitial inflammation, hyaline cast formation, acute tubular necrosis, and epithelial vacuolar degeneration.
2.9 Histopathological scoring
A pathologist used a scoring system to evaluate renal tissue damage semi-quantitatively. Tissue damage was assessed in 10 fields per section per animal, and the average score for each group was calculated for comparison. The scoring system rated damage severity from 0 to 4 as follows: 0 (no change), 1 (1-25%), 2 (26-50%), 3 (51-75%), and 4 (>75%) [27].
2.10 Statistical analysis
All data were expressed as mean ± standard deviation (SD). Statistical comparisons among groups were performed using one-way analysis of variance (ANOVA), followed by post hoc testing to determine significance levels. A p-value ≤ 0.05 was considered statistically significant.
2.11 Ethical approval
All animal procedures were conducted in accordance with the ethical guidelines for the care and use of laboratory animals and were approved by the Animal Ethics Committee of the College of Medicine, Baghdad University Approval No. [03-31]. The study adhered to internationally accepted standards for laboratory animal care and welfare.
3.1 Effect of liquiritigenin on renal function (urea and creatinine) and RML biomarkers
In the induction group, serum urea and creatinine levels significantly increased (p < 0.001) compared to the control group, confirming renal dysfunction. The vehicle group showed no significant improvement in these markers. Both LQ-treated groups (LQ30+GLY and LQ50+GLY) exhibited substantial reductions in serum urea and creatinine levels compared to the induction (p < 0.001), with the LQ50+GLY group demonstrating the most pronounced protective effect. The induction group showed a significant elevation in CK levels (p < 0.001), indicating extensive muscle injury and successful induction of RML. The vehicle group did not show a significant difference in CK levels compared to the induction group. The LQ50+GLY treated group displayed significant reductions in CK levels (p < 0.05), suggesting LQ’s role in mitigating RML-induced renal injury (Table 1, Figure 1).
Table 1. Effects of LQ on renal functions and RML parameters
|
Group |
Urea |
p-value |
Creatinine |
p-value |
CK |
p-value |
|
Control |
24.08 ± 7.66 |
<0.001a |
0.61 ± 0.2 |
<0.001a |
767.25 ± 247.63 |
<0.001a |
|
Induction |
89.16 ± 26.0 |
|
2.05 ± 0.69 |
|
2919.17±633.40 |
|
|
Vehicle |
70.37±13.53 |
0.280 |
1.93 ± 0.46 |
0.37 |
3223.42±1364.07 |
1.00 |
|
LQ30 |
34.50±11.16 |
<0.001b |
0.65 ± 0.08 |
<0.001b |
2539.08±1512.46 |
0.984 |
|
LQ50 |
32.20±6.83 |
<0.001b |
0.63 ± 0.1 |
<0.001b |
1944.88±850.68 |
<0.05b |
Data as (Mean±SD), (a) significantly different compared with control group, (b) significantly different compared with induction group.
Figure 1. Effects of LQ on renal functions and RML biomarkers (a) significantly different compared with the control group; (b) significantly different compared with the induction group
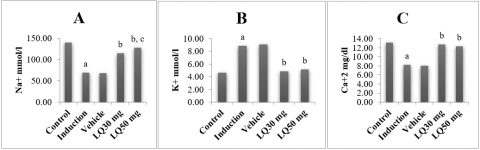
3.2 Effect of liquiritigenin on electrolytes imbalance
GLY-induced AKI led to significant electrolyte imbalances, with serum Na+ and Ca2+ levels significantly decreased (p < 0.001), while K+ levels were significantly elevated (p < 0.001) compared to the control group. Both LQ30+GLY and LQ50+GLY groups showed improvements in electrolyte balance, with significant increases in Na+ and Ca2+ levels and a significant decrease in K+ levels compared to the induction group. The LQ30+GLY group showed a significant increase in Na+ levels compared with the LQ30 group (Table 2, Figure 2).
Table 2. Effect of liquiritigenin on serum electrolyte levels
|
Group |
Sodium (mmol/l) |
p-value |
Potassium(mmol/l) |
p-value |
Calcium (mg/dl) |
p-value |
|
Control |
139.66±2.77 |
<0.001a |
4.63±0.89 |
<0.001a |
13.11±0.51 |
<0.001a |
|
Induction |
68.64±20.66 |
|
8.89±1.63 |
|
8.23±0.99 |
|
|
Vehicle |
67.80±20.04 |
0.98 |
9.06±1.46 |
0.72 |
8.04±0.96 |
0.72 |
|
LQ30 |
114.75±9.67 |
<0.001b |
4.83 ± 0.41 |
<0.001b |
12.68 ± 0.69 |
<0.001b |
|
LQ50 |
127.83 ± 3.681 |
<0.001b, <0.01c |
5.12 ± 0.8 |
<0.001b |
12.28 ± 0.58 |
<0.001b |
Data as (Mean±SD), (a) significantly different compared with control group, (b) significantly different compared with induction group.
Figure 2. Effect of liquiritigenin on serum electrolyte levels (a) significantly different compared with control group; (b) significantly different compared with induction group; (c) significantly different compared with LQ30
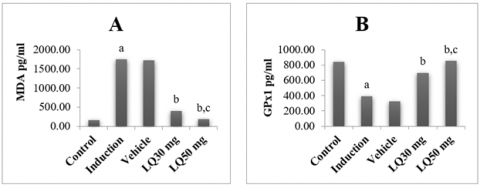
3.3 Effect of liquiritigenin on oxidative stress markers
The induction group exhibited a marked decrease in the antioxidant enzyme GPx1 (p < 0.001) and an increase in the lipid peroxidation marker MDA (p < 0.001) relative to the control group, confirming high oxidative stress levels. Treatment with LQ significantly increased GPx1 levels and reduced MDA levels in both LQ30+GLY and LQ50+GLY groups, with the LQ50+GLY group displaying the most substantial effects. These results highlight LQ’s ability to enhance antioxidant defenses and reduce oxidative damage in renal tissues (Table 3, Figure 3).
Table 3. Effect of LQ on tissue oxidative stress markers
|
Group |
GPx1 |
p-value |
MDA |
p-value |
|
Control |
844.29±83.6 |
<0.001a |
169.98±91.53 |
<0.001a |
|
Induction |
393.53±131.04 |
|
1754.22±216.97 |
|
|
Vehicle |
326.11±107.38 |
0.20 |
1719.89±260.9 |
0.81 |
|
LQ30 |
698.89±157.07 |
<0.001b |
406.99± 212.47 |
<0.001b |
|
LQ50 |
855.58±106.57 |
<0.001b, <0.01c |
191.55± 79.62 |
<0.001b, <0.01c |
Data as (Mean±SD), (a) significantly different compared with control group, (b) significantly different compared with induction group, (c) significantly different compared with LQ30
Figure 3. Effects of LQ on tissue oxidative stress markers. (a) significantly different compared with the control group; (b) significantly different compared with the induction group; (c) significantly different compared with LQ30
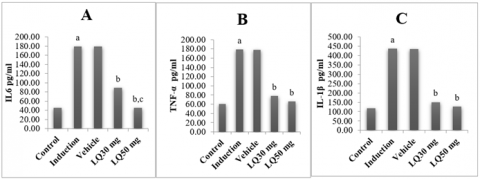
3.4 Effect of liquiritigenin on pro-inflammatory cytokines
The induction group showed significant elevation of proinflammatory cytokines IL6, TNF-α, and IL1β (p < 0.001) compared to the control group, indicating an inflammatory response associated with AKI. The vehicle group showed no significant difference from the induction group. LQ30+GLY and LQ50+GLY groups exhibited a marked reduction in these cytokines compared to the GLY-induced group (p < 0.001), with the LQ50+GLY group showing a more significant decrease in IL6. These findings suggest that LQ effectively modulates the inflammatory response in AKI (Table 4, Figure 4).
Table 4. Effect of LQ on tissue pro-inflammatory cytokines
|
Group |
IL6 (pg/ml) |
p-value |
TNF-α(pg/ml/) |
p-value |
IL1β(pg/ml/) |
p-value |
|
Control |
45.53±8.55 |
<0.001a |
60.33±19.9 |
<0.001a |
119.36±55.77 |
<0.001a |
|
Induction |
179.25±19.74 |
|
179.22±20.18 |
|
436.45±37.36 |
|
|
Vehicle |
179.25±19.74 |
1.00 |
177.59±18.92 |
0.81 |
434.45±34.54 |
0.91 |
|
LQ30 |
88.97±24.70 |
<0.001b |
78.17± 16.61 |
<0.001b |
150.90±43.59 |
<0.001b |
|
LQ50 |
45.53±18.55 |
<0.001b, <0.001c |
66.11 ± 14.5 |
<0.001b |
126.36±54.80 |
<0.001b |
Data as (Mean±SD), (a) significantly different compared with control group, (b) significantly different compared with induction group, (c) significantly different compared with LQ30
Figure 4. Effect of LQ on tissue pro-inflammatory cytokines. (a) significantly different compared with the control group; (b) significantly different compared with the induction group; (c) significantly different compared with LQ30
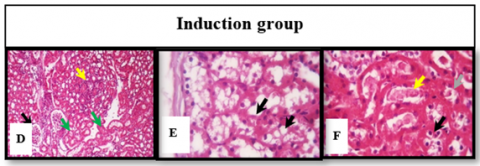
3.5 Histopathological analysis of renal tissue
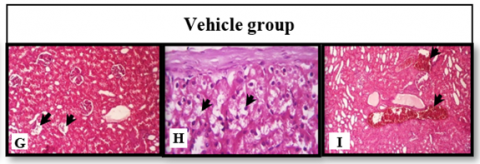
Histopathological examination of renal tissues revealed significant structural damage in the GLY-induced AKI and Vehicle groups, while the LQ-treated groups demonstrated varying degrees of renal protection. The primary pathological features observed included tubular necrosis, glomerular congestion, interstitial inflammation, and hyaline cast formation, as summarized in Table 5 and illustrated in Figure 5. In the control group (Figure 5(A-C)), the kidney appears within normal limits, A: normal glomeruli (black arrow) and normal proximal (blue arrow) and distal (green arrow), B: normal subcapsular renal tubules (black arrow). C: normal proximal renal tubular epithelium (black arrow), normal interstitial capillaries (blue arrow). In the induction group (Figure 5(D-F)), D: glomerular atrophy (black arrow), hyaline degeneration of renal tubules (red arrow), protein cast (green arrow) in the cortical renal tubules, and interstitial inflammation (yellow arrow). E: marked vacuolation of the renal tubular epithelium of the sub-capsular region (black arrow). F: marked vacuolation of renal tubular (black arrow), hyaline degeneration of cortical renal tubules (red arrow), and protein cast in both proximal (green arrow) and distal (yellow arrow). This group showed a significant difference from the control group (P ≤ 0.05). Similar results were seen in the vehicle-treated group (Figure 5(G-I)), G: marked vacuolation of renal tubular epithelium in the sub-capsular region (black arrow). H: renal vascular congestion (black arrow) I: interstitial inflammation (black arrow). This group shows no statistically significant differences from the induction group (P ≥ 0.05).
Marked improvement of renal changes was seen in the LQ (30 mg), in which this group showed significant (p≤0.05) differences regarding all study parameters compared to the induction group Figure 5(J-L). J: some atrophic glomeruli (black arrow) vacuolation of renal tubular epithelium in all proximal (blue arrow) and distal (green arrow) tubules in the cortex, with mild protein aggregates in the renal tubules (yellow arrow). K: glomerular congestion (black arrow) vacuolation of renal tubular epithelium in all proximal (blue arrow) and distal (green arrow) tubules in the cortex, with mild protein aggregates in the renal tubules (yellow arrow). L: vacuolation of medullary renal tubular epithelium (blue arrow), with protein cast in the renal tubules (yellow arrow). The treated liquiritigenin (50 mg) group showed superior renal improvements in Figure 5(M-O). M: It shows normal glomeruli (black arrow) and normal proximal (blue arrow) and distal (green arrow) renal tubules. N: normal subcapsular renal tubular epithelium (black arrow) in the cortex. O: normal glomerulus (black arrow) and mild hyaline degeneration of the proximal (blue arrow) tubules. This group showed a marked reduction in all changes seen in the other groups. The kidney showed marked restoration of renal structural normalcy, in which this group had no statistical differences from the control group except for the hyaline cast. In comparison with induction, liquiritigenin (50 mg) showed significant differences (P≤0.05) in the improvement of renal function. All of the said parameters were scored. All scoring parameters are shown in Table 5.
Figure 5. Histopathological findings in the study groups
The kidney section of the control group (A-C), The kidney section of the induction group (D-F), The kidney section of the vehicle group (G-I), The kidney section of the LQ30-treated group (J-K), The kidney section of the LQ50 treated group (M-O). (A, D, G, I, L, M. 10X). (B, C, E, F, H, J, K, N, O 40X).
Table 5. The averages of histopathological changes
|
Pathological Changes |
Control (score) |
Vehicle (score) |
Induction score |
LQ 30%(score) |
LQ 50% (score) |
|
Inflammation |
0 (0) |
69±3.41 a (3) |
62±1.45 a (3) |
62±1.45 (3) |
0 b (0) |
|
Glomerular atrophy |
0 (0) |
81±0.15 a (4) |
77±0.93 a (4) |
14±1.22 b (1) |
0 b (0) |
|
Glomerular congestion |
0 (0) |
93±0.09 a (4) |
81±2.4 a (4) |
30±2.39 b (2) |
0 b (0) |
|
Epithelial hyaline degeneration |
0 (0) |
89±4.63 a (4) |
93±3.1 a (4) |
26±0.89 b (2) |
9±1.62 b (1) |
|
Epithelial vacuolar degeneration |
0 (0) |
82±2.77 a (4) |
82±1.11 a (4) |
29±3.74 b (2) |
4±1.51 b (1) |
|
Hyaline cast formation |
0 (0) |
91±0.4 a (4) |
95±0.83 a (4) |
26±0.8 b (2) |
27±0.2 b (2) |
|
Interstitial vascular congestion |
0 (0) |
65±5.54 a (4) |
69 ±4.12 a (3) |
5±3.3 b (1) |
0 b (0) |
The values are expressed as a mean± standard deviation (SD); (a) refers to significant changes (p ≤ 0.05) compared with the control group. (b) refers to significant changes (p ≤ 0.05) compared with the induction group.
Phytomedicines are efficient, stunning products with global attentiveness in consideration of their therapeutic effects, widely available sources, and affordable cost compared with chemical medicines [28]. Polyphenols, specifically flavonoids, are widely investigated in several studies using the GLY model to induce myoglobinuric- AKI due to their anti-inflammatory, antioxidant, and antiapoptotic properties [29]. GLY-induced myoglobinuric-AKI is the most frequently used model to study AKI and predict a novel treatment. It shows a remarkable similarity of renal failure induced by myoglobinuria in humans due to traumatic injury or extensive muscle workouts [30].
Renal vasoconstriction, ischemic injury, tubular occlusion due to Mb cast formation, Mb-induced oxidative stress, and inflammation are the primary pathological mechanisms of GLY-induced AKI. Vasoconstriction, a characteristic feature of AKI evoked by GLY, is mediated by the release of several vasoconstrictors, including (AngП, vasopressin, MDA, endothelin, and TNF-α), due to reduced intravascular fluids after diffusion into raptured muscles, Mb nephrotoxicity, and inflammation, consequently lead to renal hypoperfusion and reduces glomerular filtration rate (GFR). At this time, vasoconstriction decreases the tubular fluids, which is considered a proper medium for Mb cast formation, causing tubular occlusion and aggravating the reduction in the GFR [31]. The previous factors, plus structural damage of kidney tissues, such as diminishing brush borders and tubular necrosis, lead to the impairment of kidney excretory function, causing the accumulation of nitrogenous waste products [32]. Additionally, elevation in serum creatinine is attributed to RML as injured muscle releases a vast amount of creatinine [33]. Our results exhibited a marked elevation in renal function biomarkers (urea and creatinine), in addition to CK levels, in the induction group, which confirms the induction of RML and subsequent AKI incidence because the significant elevation in serum CK, an indicator of RML, meanwhile, elevation in urea and creatinine levels reflect a primary manifestation of AKI [34]. Supported by GLY-Mediated histopathological alteration in renal tissues, including tubular necrosis, hyalin degeneration, tubular cast formation, and glomerular atrophy.
The earlier results align with the current study's findings, which reported similar biochemical and histopathological changes after administering the GLY solution [24]. The vehicle-treated group didn’t produce any significant changes compared with the induction group, which was attributed to the absence of protective effects of the vehicle Solution. In contrast, LQ-treated groups showed a significant reduction in renal function parameters (urea and creatinine) and CK levels, compared with the induction group, as well as attenuation of histological changes, as the LQ-treated groups significantly improved the structural changes presented in the GLY group, suggesting possible renoprotective effects, mitigated GLY-mediated AKI as well as attenuating the RML progressing in a previous study showed a remarkable reduction in both urea and creatinine levels in the cisplatin-induced AKI model, which supports our findings [22].
The current study's results were compatible with those of Yousef et al. [35]. They reported that Licorice (Glycyrrhiza glabra) extract exhibited nephroprotective activity against gentamicin-induced nephrotoxicity. The results showed its ability to improve renal function by a significant reduction of urea and creatinine [35]. Nassan et al. [36] reported the nephroprotective effect of Glycyrrhiza glabra against gentamicin-induced renal damage via inhibiting proinflammatory mediators and enhancing antioxidant enzymes, scavenging ROS, and restoring normal renal function. The ability of LQ to restore normal renal function may be explained by its blocking effect against the angiotensin enzyme, which in turn blocks angiotensin-mediated renal vasoconstriction [37]. In addition to LQ's free radical scavenging properties, they inhibit lipid peroxidation of renal tubular cells and the formation of potent vasoconstrictors like MDA and isoprostane F2, which enhance renal blood flow [38].
AKI causes a disturbance in the water and electrolytes homeostasis related to a reduction in GFR [39]. The present study's findings revealed a significant decrease in serum Na+ level in the induction and vehicle groups that received GLY, compared with the control group, attributed to tubular damage leading to reabsorption impairment. Our results were compatible with the findings of previous studies that exhibited a significant reduction in serum Na+ level in the rats model of GLY-induced RML and an increase in fractional Na+ excretion [18, 40]. Contrary to our findings, many studies reported a significant increase in serum Na+ level after GLY administration, which may be attributed to hypovolemia and the hypertonicity of the GLY solution, in addition to fluid restriction as a compensatory renal mechanism to overcome hypovolemia. This also may be attributed to ATN, which results in a decline in the kidney's functional units. This action will stimulate the multiple compensatory mechanisms in the hyper-functioning remaining nephrons, most notably the augmented rates of Na+ reabsorption that led to hypernatremia [41, 42].
The LQ (30,50) treatment groups reveal a significant increase in Na+ levels, the highest improvement seen with the LQ 50 mg dose. The LQ (30,50) treatment groups significantly reduced K+ levels, reflecting the LQ renoprotective effects. On the other hand, GLY administration exhibited a marked increase in serum K+ in the induction and vehicle groups. The previous studies showed elevated serum K+ levels in the animals that received GLY injections, which is consistent with our findings [12, 43]. Due to muscle breakdown, Hyperkalemia usually manifests as electrolytes disturbances associated with RML. Hyperkalemia may cause severe cardiac complications, specifically arrhythmia, that must be managed as soon as possible [43]. Hyperkalemia is also attributed to reduced urine output, decreasing K+ excretion [44]. The ability of LQ to reverse Na+ and K+ levels may be attributed to the mineralocorticoid action of licorice active constituent, which preserves Na+ and water and releases K+ in the urine, which may help reverse the hyperkalemia and hyponatremia associated with RML [38, 45]. Moreover, studies have demonstrated that flavonoids could effectively ameliorate electrolyte disturbances associated with GLY-induced AKI [46]. In addition, the ability of LQ to retrieve normal kidney function can reverse the electrolyte disturbances as it enhances the filtration and reabsorption mechanisms. At the same time, Ca2+ levels in the induction and vehicle groups significantly decreased with no significant changes between the two groups, which is consistent with the findings of earlier investigators. This hypocalcemia is attributed to the trapping of Ca2+ intracellularly in the early stage of AKI (oliguric phase); studies have shown that hypocalcemia is temporary at the beginning stage of RML, as the Ca2+ diffused after muscle breakdown, which may result in hypercalcemia [47]. LQ treatment groups reversed the hypocalcemia seen in the induction group significantly.
Numerous investigators have mentioned the role of inflammation and oxidative stress in the pathogenesis of GLY-induced AKI. These studies reported that pro-inflammatory cytokines and ROS significantly initiate and develop AKI due to the Mb nephrotoxic effects. Accordingly, inflammation and oxidative stress are considered the primary therapeutic targets in earlier studies to manage AKI stimulated by GLY [12]. In this study, renal tissue oxidative stress markers (MDA, GPx1) showed significant changes compared with the control group; MDA was significantly high, while GPx1 was significantly low, reflecting that oxidative stress causes lipid peroxidation and depletion of antioxidant enzymes. These results were compatible with previous research, which reported comparable results regarding oxidative stress markers [42, 46]. The treatment groups showed significant changes in these markers, as LQ reduced tissue MDA level and elevated tissue GPx1 compared with the induction group and in a dose-dependent manner. Previously, LQ exhibited the same results in modulating oxidative stress markers against liver damage triggered by carbon tetrachloride [48]. Several factors generated ROS, producing oxidative stress like muscle disintegration-induced systemic inflammation, ischemic reperfusion injury, and myoglobin-derived free iron. Updated evidence reported the role of iron overload in GLY-AKI through ferroptosis, a different form of tubular epithelial cell death due to iron trapping-mediated lipid peroxidation [49]. LQ chiral flavonoids with a simple structure in comparison with quercetin and resveratrol have good bioavailability; it’s an estrogen-agonist activity, which enhances its antioxidant efficacy via activation of endogenous antioxidant enzymes production like GPx1 and SOD effects, NF-κB suppression effect that attenuates inflammatory-mediated ROS liberation and free radical scavenging. In contrast, other antioxidants possess the antioxidant only through radical scavenging [14, 38, 50]. Moreover, polyphenols, particularly flavonoids, have astonishing free radical scavenging properties through electron donation or hydrogen atom transfer. They make radical species more stable and have chelating effects that could alleviate iron-derived ROS [46]. Interestingly, the OH· scavenging properties of LQ could be of high value in mitigating renal tissue MDA levels due to the significant role of this radical in the peroxidation of tubular cells, elevating MDA values [20, 38]. Advanced evidence suggested that LQ could mitigate AKI by inhibiting ferroptosis through VKORC1 action and reducing oxidative stress markers; therefore, the reduced MDA level by LQ could be related to this effect, which supports our results [23]. Moreover, the capability of LQ to enhance the antioxidant enzyme GPX may be related to its ability to stimulate the nuclear factor euthyroid-2-related factor 2 (Nrf2), which is a transcription factor with high value in the regulation of antioxidant enzymes involved in the restoration of redox balance during stress conditions, thus restoring mitochondrial integrity [51]. It was reported that LQ stimulates this factor, which in turn replenishes the tissue content of various antioxidant enzymes, including GPx1, that attenuate oxidative stress and prevent cellular damage [52]. In response to harmful exciters like trauma, toxic damage, oxidative stress that induce T-lymphocytes, macrophages, myoglobinuria, and ischemic injury, inflammation develops by releasing several pro-inflammatory mediators. It may lead to severe complications, particularly in acute case response [53, 54]. The pro-inflammatory cytokines (IL1β, IL6, TNF-α) are the central cytokines involved in the pathogenesis of AKI induced by GLY. They stimulate inflammation and exacerbate AKI by causing cellular damage and promoting leukocyte infiltration. In the current study, cytokines (IL1β, IL6, and TNF-α) were markedly elevated in the induction group, highlighting an inflammatory response associated with AKI; these findings were in line with the earlier research, which showed an elevation in renal tissue levels of these cytokines [28, 47, 55]. The vehicle group showed no significant change compared with the induction group, reflecting that solvent has no effects on inflammatory markers. At the same time, the LQ50 treatment group exhibited no significant difference from the LQ30 group except for IL6, which showed a dose-dependent reduction.
Studies mentioned the significant role of TNF-α in GLY-induced AKI pathogenesis; it is stimulated rapidly after GLY administration, induces immune cell infiltration, traps neutrophils, and aggravates the secretion of other cytokines. The released TNF-α can amplify inflammatory response through its activation impact on nuclear factor kappa b (NF-κB). This factor regulates the expression of several pro-inflammatory cytokines; consequently, its activation leads to transcribing stimulation of its downstream cytokines (IL6, IL1β, TNF-α). Evidence has shown that mitigating TNF-α can protect against GLY-AKI [47, 56]. In addition, oxidative stress, evoked by Mb and other toxic materials released from damaged muscles, stimulates NF-κB, thereby enhancing the expression of pro-inflammatory cytokines [31]. Similarly, studies mentioned the pivotal impact of (IL1β and IL6) in the development of AKI due to GLY administration, which is released in response to inflammation of renal tissues and infiltrated immune cells. It has been shown that IL6 serum levels directly reflect the severity of renal damage [57, 58].
Several previous studies have reported the inflammatory suppression action of LQ and licorice-active constituents by suppressing the NF-κB signaling pathway, inhibiting cytokine production such as TNF-α and IL6 [59, 60]. Moreover, evidence supports the anti-inflammatory role of LQ in modulating the cytokines induced by lipopolysaccharides' effects on microglial cells and in the hydrogen peroxide–exposed mouse [61]. In addition, LQ can mitigate inflammation-induced cartilage damage in rats by inhibiting TNF-α and IL1β [62]. LQ mitigated the pro-inflammatory cytokines involved in the pathogenesis of diabetic nephropathy by suppressing NF-κB and nodi-like protein 3 (NLRP3) inflammasome pathway [63]. Oxidative stress and inflammation are interchangeable; they stimulate each other. Previously mentioned antioxidant and anti-inflammatory effects can inhibit this vicious circle by suppressing gene expression of IL1β, IL6, and TNF-α [64]. Therefore, inhibiting NF-κB, NLRP3, and antioxidant effects of LQ could explain pro-inflammatory markers reduction in the current study. Histopathological evaluations provided concrete evidence of the structural preservation afforded by LQ. In the GLY-induced AKI and vehicle groups, severe tubular necrosis, glomerular atrophy, and interstitial inflammation were observed, reflecting profound renal damage. LQ treatment, especially at the 50 mg/kg dose, minimized these histological alterations, as evidenced by minimal necrosis, preserved glomerular structure, and reduced inflammation. These findings underscore LQ’s potential to prevent myoglobin-induced oxidative stress, limit leukocyte infiltration, and mitigate structural degradation in renal tissue. Similar nephroprotective agents, such as magnesium isoglycyrrhizinate, an active constituent of licorice roots, have demonstrated comparable effects, reducing renal injury by lowering ROS production and dampening inflammatory responses [65].
This work confirms the high nephroprotective activity of LQ against glycerol-induced AKI in rabbits. Our data indicate that LQ, at the higher dosage of 50 mg/kg, significantly reduced renal dysfunction parameters, urea and creatinine, from 89.16 ± 26.0 to 32.20 ± 6.83 mg/dl and from 2.05 ± 0.69 to 0.61 ± 0.1 mg/dl, respectively. It also reversed oxidative stress markers, MDA and GPX, from 1754.22 ± 216.97 to 191.55 ± 79.62 pg/ml and from 393.53 ± 131.04 to 855.58 ± 106.57 pg/ml, respectively, and inflammatory markers (IL-6, TNF-α, and IL-1β), from 179.25 ± 19.74 to 45.53 ± 18.55 pg/ml, from 179.22 ± 20.18 to 66.11 ± 14.5 pg/ml, and from 436.45 ± 37.36 to 126.36 ± 54.80 pg/ml, respectively. These markers are key actors in AKI pathophysiology, especially in forms related to RML.
LQ, a flavonoid extracted from licorice roots, substantially attenuates RML-associated AKI by inhibiting the main pathological mechanisms involving pro-inflammatory cytokines (mainly TNF-α, IL-6, and IL-1β) and oxidative stress-mediated cellular injury, with notable improvements in renal tissue architecture. LQ could be one of the most promising and effective alternatives to conventional AKI treatments.
Future studies are necessary to elucidate its molecular mechanisms, perform a detailed assessment of its safety profile, and consider clinical applications for AKI management. The study lays the foundation for LQ's furtherance toward its potential therapeutic application in the prevention and mitigation of renal damage in patients with AKI, especially those at high risk of RML-induced kidney injury.
Male rabbits were selected for their physiological similarities to humans regarding kidney structure and injury response. However, inherent differences may affect the translatability of Liquiritigenin’s (LQ) nephroprotective effects on human AKI cases. Further studies, particularly in human renal tissue models or clinical trials, are needed to confirm the relevance of these findings in human patients.
This study utilized a glycerol-induced AKI model, mainly mimicking rhabdomyolysis-associated AKI. While LQ demonstrated efficacy in this context, its effectiveness in other forms of AKI, such as those caused by sepsis, ischemia-reperfusion, or nephrotoxic drugs, remains unknown. Testing LQ in various AKI models could provide a more comprehensive understanding of its potential as a general nephroprotective agent.
The study investigated only two doses of LQ (30 mg/kg and 50 mg/kg), which may not fully represent the optimal therapeutic range for maximum efficacy and safety. Expanding the study to include a broader range of doses would help determine the minimum effective dose and evaluate any possible toxicity at higher levels, aiding in the establishment of a safer dosing profile for future applications.
This work was supported by the staff of the Basra College of Medicine animal facility, who provided animal care and housing throughout the study. We also acknowledge the valuable assistance the College of Medicine, university of Baghdad provided for guidance on ethical protocols.
[1] Makris, K. (2018). The role of the clinical laboratory in the detection and monitoring of acute kidney injury. Journal of Laboratory and Precision Medicine, 3: 69. https://doi.org/10.21037/jlpm.2018.07.06
[2] Bonventre, J.V. (2008). Pathophysiology of acute kidney injury. Nephrology Rounds, 6(7): 13-20.
[3] Fu, Z., Hao, X., Lv, Y., Hong, Q., Feng, Z., Liu, C. (2024). Effect of electronic alerts on the care and outcomes in patients with acute kidney injury: A meta-analysis and trial sequential analysis. BMC Medicine, 22: 408. https://doi.org/10.1186/s12916-024-03639-x
[4] Nasr, A.M., Rezq, S., Shaheen, A., Elshazly, S.M. (2020). Renal protective effect of nebivolol in rat models of acute renal injury: Role of sodium-glucose co-transporter 2. Pharmacological Reports, 72: 956-968. https://doi.org/10.1007/s43440-020-00059-5
[5] Kung, C.W., Chou, Y.H. (2023). Acute kidney disease: An overview of the epidemiology, pathophysiology, and management. Kidney Research and Clinical Practice, 42(6): 686-699. https://doi.org/10.23876/j.krcp.23.001
[6] Darmon, M., Ostermann, M., Cerda, J., Dimopoulos, M. A., et al. (2017). Diagnostic work-up and specific causes of acute kidney injury. Intensive Care Medicine, 43: 829-840. https://doi.org/10.1007/s00134-017-4799-8
[7] Jensen, S.K., Heide-Jørgensen, U., Gammelager, H., Birn, H., Christiansen, C.F. (2024). Acute kidney injury duration and 20-year risks of CKD and cardiovascular disease. Kidney International Reports, 9(4): 817-829. https://doi.org/10.1016/j.ekir.2024.01.034
[8] Gupta, A., Thorson, P., Penmatsa, K.R., Gupta, P. (2021). Rhabdomyolysis: revisited. The Ulster Medical Journal, 90(2): 61-69.
[9] Al-Windawi, S., Ali, A. (2013). Rhabdomyolysis associated AKI: Case series from Iraq. Journal of the Faculty of Medicine Baghdad, 55(2): 186-189.
[10] Torres, P.A., Helmstetter, J.A., Kaye, A.M., Kaye, A.D. (2015). Rhabdomyolysis: pathogenesis, diagnosis, and treatment. Ochsner Journal, 15(1): 58-69.
[11] Chavez, L.O., Leon, M., Einav, S., Varon, J. (2016). Beyond muscle destruction: A systematic review of rhabdomyolysis for clinical practice. Critical Care, 20: 135. https://doi.org/10.1186/s13054-016-1314-5
[12] Wang, Q., Qi, G., Zhou, H., Cheng, F., Yang, X., Liu, X., Wang, R. (2023). Protective effect of thymol on glycerol-induced acute kidney injury. Renal Failure, 45(1): 2227728. https://doi.org/10.1080/0886022X.2023.2227728
[13] Hebert, J.F., Burfeind, K.G., Malinoski, D., Hutchens, M.P. (2023). Molecular mechanisms of rhabdomyolysis-induced kidney injury: From bench to bedside. Kidney International Reports, 8(1): 17-29. https://doi.org/10.1016/j.ekir.2022.09.026
[14] Kim, Y.W., Zhao, R.J., Park, S.J., Lee, J.R., Cho, I.J., Yang, C.H., Kim, S.G., Kim, S.C. (2008). Anti-inflammatory effects of liquiritigenin as a consequence of the inhibition of NF-κB‐dependent iNOS and proinflammatory cytokines production. British Journal of Pharmacology, 154(1): 165-173. https://doi.org/10.1038/bjp.2008.79
[15] Wu, S., Pang, Y., He, Y., Zhang, X., Peng, L., Guo, J., Zeng, J. (2021). A comprehensive review of natural products against atopic dermatitis: Flavonoids, alkaloids, terpenes, glycosides and other compounds. Biomedicine & Pharmacotherapy, 140: 111741. https://doi.org/10.1016/j.biopha.2021.111741
[16] Jain, R., Hussein, M.A., Pierce, S., Martens, C., Shahagadkar, P., Munirathinam, G. (2022). Oncopreventive and oncotherapeutic potential of licorice triterpenoid compound glycyrrhizin and its derivatives: Molecular insights. Pharmacological Research, 178: 106138. https://doi.org/10.1016/j.phrs.2022.106138
[17] Zhou, M., Dai, Y., Ma, Y., Yan, Y., Hua, M., Gao, Q., Geng, X. and Zhou, Q. (2022). Protective effects of liquiritigenin against cisplatin-induced nephrotoxicity via NRF2/SIRT3-mediated improvement of mitochondrial function. Molecules, 27(12): 3823. https://doi.org/10.3390/molecules27123823
[18] Guo, R.Z., Li, J., Pan, S.K., Hu, M.Y., Lv, L.X., Feng, Q., Qiao, Y.J., Duan, J.Y., Liu, D.W., Liu, Z.S. (2024). Liquiritigenin, an active ingredient of liquorice, alleviates acute kidney injury by VKORC1-mediated ferroptosis inhibition. The American Journal of Chinese Medicine, 52(5): 1507-1526. https://doi.org/10.1142/S0192415X24500599
[19] Gondal, A.Z., Foris, L.A., Zubair, M., Richards, J.R. (2023). Serum Myoglobin. StatPearls Publishing.
[20] Williams, J.D., Kumar, R., Afolabi, J.M., Park, F. and Adebiyi, A. (2023). Rhabdomyolysis aggravates renal iron accumulation and acute kidney injury in a humanized mouse model of sickle cell disease. Free Radical Research, 57(6-12): 404-412. https://doi.org/10.1080/10715762.2023.2269313
[21] Oyagbemi, A.A., Adejumobi, O.A., Ajibade, T.O., Asenuga, E.R., Afolabi, J.M., Ogunpolu, B.S., Falayi, O.O., Hassan, F.O., Nabofa, E.W., Olutayo Omobowale, T., Ola-Davies, O.E. (2021). Luteolin attenuates glycerol-induced acute renal failure and cardiac complications through modulation of kim-1/NF-κB/Nrf2 signaling pathways. Journal of Dietary Supplements, 18(5): 543-565. https://doi.org/10.1080/19390211.2020.1811442
[22] Salih, S.M., Adam, S.A. (2024). Imbalance of Pro and anti-inflammatory cytokines in rheumatoid arthritis in Iraqi patients. Journal of the Faculty of Medicine Baghdad, 66(3): 388-392.
[23] Al Asmari, A.K., Al Sadoon, K.T., Obaid, A.A., Yesunayagam, D. and Tariq, M. (2017). Protective effect of quinacrine against glycerol-induced acute kidney injury in rats. BMC Nephrology, 18: 1-10. https://doi.org/10.1186/s12882-017-0450-8
[24] Hareedy, M.S., Abdelzaher, L.A., Badary, D.M., Alnasser, S.M., Abd-Eldayem, A.M. (2021). Valproate attenuates hypertonic glycerol-induced rhabdomyolysis and acute kidney injury. Néphrologie & Thérapeutique, 17(3): 160-167. https://doi.org/10.1016/j.nephro.2020.12.003
[25] Flecknell, P. (2023). Laboratory Animal Anaesthesia and Analgesia. Academic Press.
[26] Suvarna, S.K., Layton, C., Bancroft, J.D. (2018). Bancroft's Theory and Practice of Histological Techniques. Elsevier Health Sciences.
[27] Kuttancheri, T., Das, S.K., Shetty, M.S., Satish, S., Bathrenathh, B. (2023). Renal resistive index as a marker of histopathological damage in diabetic and non-diabetic chronic kidney disease. Egyptian Journal of Radiology and Nuclear Medicine, 54(1): 159. https://doi.org/10.1186/s43055-023-01096-9
[28] Amirshahrokhi, K. (2021). Thalidomide reduces glycerol‐induced acute kidney injury by inhibition of NF-κB, NLRP3 inflammasome, COX-2 and inflammatory cytokines. Cytokine, 144: 155574. https://doi.org/10.1016/j.cyto.2021.155574
[29] Yin, M., Jiang, N., Guo, L., Ni, Z., Al-Brakati, A.Y., Othman, M.S., Moneim, A.E.A., Kassab, R.B. (2019). Oleuropein suppresses oxidative, inflammatory, and apoptotic responses following glycerol-induced acute kidney injury in rats. Life Sciences, 232: 116634. https://doi.org/10.1016/j.lfs.2019.116634
[30] Ramadhan, M.A., Al-Saedi, H.F., Ismaeel, G.L. and Hussein, U.A.R. (2020). The possible nephroprotective effect of roflumilast ameliorating glycerol-induced myoglobinuric acute renal injury in rabbits model. Indian Journal of Forensic Medicine & Toxicology, 14(4): 3326-3332.
[31] Hussein, Z.T., Hussein, A.A. (2024). The potential renoprotective effects of ticagrelor in rhabdomyolysis-induced acute kidney injury in rat. Maaen Journal for Medical Sciences, 3(3): 7. https://doi.org/10.55810/2789-9136.1054
[32] Khwaja, A. (2012). KDIGO clinical practice guidelines for acute kidney injury. Nephron Clinical Practice, 120(4): 179-184. https://doi.org/10.1159/000339789
[33] Komada, T., Usui, F., Kawashima, A., Kimura, H., Karasawa, T., Inoue, Y., Kobayashi, M., Mizushina, Y., Kasahara, T., Taniguchi, S.I. and Muto, S. (2015). Role of NLRP3 inflammasomes for rhabdomyolysis-induced acute kidney injury. Scientific Reports, 5(1): 10901. https://doi.org/10.1038/srep10901
[34] Naderi, E., Rad, A.K., Nazari, S., Khazaei, M., Shahraki, S., Hosseinian, S. (2022). Nigella sativa and its main constituent, thymoquinone protect against glycerol-induced acute kidney injury in rats. Avicenna Journal of Phytomedicine, 12(6): 638-648. https://doi.org/10.22038/AJP.2022.20921
[35] Yousef, F.M., Alkreathy, H. (2016). Effect of licorice extract against gentamicin-induced nephrotoxicity in male rats. Life Science Journal, 13(2). https://doi.org/10.7537/marslsj13021615.
[36] Nassan, M.A., Soliman, M.M., Aldhahrani, A., Althobaiti, F., Alkhedaide, A.Q. (2021). Ameliorative impacts of Glycyrrhiza glabra root extract against nephrotoxicity induced by gentamicin in mice. Food Science & Nutrition, 9(7): 3405-3413. https://doi.org/10.1002/fsn3.2183
[37] Li, H., Zhang, Y., Dai, G., Zhaxi, C., Wang, Y., Wang, S. (2023). Identification and quantification of compounds with Angiotensin-converting enzyme inhibitory activity in licorice by UPLC-MS. Food Chemistry, 429: 136962. https://doi.org/10.1016/j.foodchem.2023.136962
[38] Ramalingam, M., Kim, H., Lee, Y., Lee, Y.I. (2018). Phytochemical and pharmacological role of liquiritigenin and isoliquiritigenin from radix glycyrrhizae in human health and disease models. Frontiers in Aging Neuroscience, 10: 348. https://doi.org/10.3389/fnagi.2018.00348
[39] Khudhair, A., Naama, K.Z.N., Khaleel, A., Saadi, Y. (2023). Acute kidney injury in neonates: A single-center experience. Journal of the Faculty of Medicine Baghdad, 65(3): 150-155. https://doi.org/10.32007/jfacmedbagdad.2048
[40] Kaya, O., Aydogdu, N., Tastekin, E., CH, K., Gunduz, O., Sut, N. (2013). Effects of losartan on glycerol-induced myoglobinuric acute renal failure in rats. Kafkas Üniversitesi Veteriner Fakültesi Dergisi, 19(2).
[41] Najafzadeh, H., Razijalali, M., Morovvati, H., Navvabi, L. (2011). Evaluation the effect of cimetidine, estradiol and vitamin E on myoglobinuric renal toxicity in rats. American-Eurasian Journal of Toxicological Sciences, 3(3): 177-183.
[42] Abugomaa, A., Elbadawy, M. (2020). Olive leaf extract modulates glycerol-induced kidney and liver damage in rats. Environmental Science and Pollution Research, 27: 22100-22111. https://doi.org/10.1007/s11356-020-08371-6
[43] Shooshtari, M.K., Sarkaki, A., Rashno, M., Hoseinynejad, K. (2024). Renal protection by ellagic acid in a rat model of glycerol-induced acute kidney injury. Veterinary Research Forum, 15(2): 105-111. https://doi.org/10.30466/vrf.2023.2000658.3859
[44] Diniz, L.R.L., Souza, M.T.D.S., Duarte, A.B.S., Sousa, D.P.D. (2020). Mechanistic aspects and therapeutic potential of quercetin against COVID-19-associated acute kidney injury. Molecules, 25(23): 5772. https://doi.org/10.3390/molecules25235772
[45] Ceccuzzi, G., Rapino, A., Perna, B., Costanzini, A., Farinelli, A., Fiorica, I., Marziani, B., Cianci, A., Rossin, F., Cesaro, A.E., Spampinato, M.D. (2023). Liquorice toxicity: A comprehensive narrative review. Nutrients, 15(18): 3866. https://doi.org/10.3390/nu15183866
[46] Kassab, R.B., Elhenawy, A.A., AbdulrahmanTheyab, Hawsawi, Y.M., Al-Amer, O.M., Oyouni, A.A.A., Habotta, O.A., Althagafi, H.A., Alharthi, F., Lokman, M.S., Alsharif, K.F. (2023). Modulation of inflammatory, oxidative, and apoptotic stresses mediates the renoprotective effect of daidzein against glycerol-induced acute kidney injury in rats. Environmental Science and Pollution Research, 30(56): 119016-119033. https://doi.org/10.1007/s11356-023-30461-4
[47] Eltahir, H.M., Elbadawy, H.M., Alalawi, A., Aldhafiri, A.J., Ibrahim, S.R., Mohamed, G.A., Shalkami, A.G.S., Almikhlafi, M.A., Albadrani, M., Alahmadi, Y., Abouzied, M.M. (2023). Alpha-Mangostin ameliorates acute kidney injury via modifying levels of circulating TNF-α and IL-6 in glycerol-induced rhabdomyolysis animal model. Acta Biochimica Polonica, 70(2): 277-284. https://doi.org/10.18388/abp.2020_6509
[48] Zhang, Y., He, Y., Yu, H., Ma, F., Wu, J., Zhang, X. (2015). Liquiritigenin protects rats from carbon tetrachloride induced hepatic injury through PGC‐1α pathway. Evidence‐Based Complementary and Alternative Medicine, 2015(1): 649568. https://doi.org/10.1155/2015/649568
[49] Qiao, O., Wang, X., Wang, Y., Li, N., Gong, Y. (2023). Ferroptosis in acute kidney injury following crush syndrome: A novel target for treatment. Journal of Advanced Research, 54: 211-222. https://doi.org/10.1016/j.jare.2023.01.016
[50] Zeng, Y., Song, J., Zhang, M., Wang, H., Zhang, Y., Suo, H. (2020). Comparison of in vitro and in vivo antioxidant activities of six flavonoids with similar structures. Antioxidants, 9(8): 732. https://doi.org/10.3390/antiox9080732
[51] He, F., Ru, X.L., Wen, T. (2020). NRF2, a transcription factor for stress response and beyond. International Journal of Molecular Sciences, 21(13): 4777. https://doi.org/10.3390/ijms21134777
[52] Shi, M., Zhang, J., Li, M., Zhao, Y., Guo, Y., Xu, J., Liu, R., Li, Z., Ren, D., Liu, P. (2023). Liquiritigenin confers liver protection by enhancing NRF2 signaling through both canonical and non-canonical signaling pathways. Journal of Medicinal Chemistry, 66(16): 11324-11334. https://doi.org/10.1021/acs.jmedchem.3c00815
[53] Panizo, N., Rubio-Navarro, A., Amaro-Villalobos, J.M., Egido, J., Moreno, J.A. (2015). Molecular mechanisms and novel therapeutic approaches to rhabdomyolysis-induced acute kidney injury. Kidney and Blood Pressure Research, 40(5): 520-532. https://doi.org/10.1159/000368528
[54] Wahid, H.H.A., Turki, K.M., AI-Tharb, A.Y. (2006). Interleukin-6 Level in serm of Iraqi patients on maintenance hemodialysis therapy. Journal of the Faculty of Medicine Baghdad, 48(4): 431-434.
[55] Guerrero‐Hue, M., García‐Caballero, C., Palomino‐Antolín, A., Rubio‐Navarro, A., Vázquez‐Carballo, C., Herencia, C., Martín‐Sanchez, D., Farré‐Alins, V., Egea, J., Cannata, P., Praga, M. (2019). Curcumin reduces renal damage associated with rhabdomyolysis by decreasing ferroptosis‐mediated cell death. The FASEB Journal, 33(8): 8961-8975. https://doi.org/10.1096/fj.201900077R
[56] Shulman, L.M., Yuhas, Y., Frolkis, I., Gavendo, S., Knecht, A., Eliahou, H.E. (1993). Glycerol induced ARF in rats is mediated by tumor necrosis factor-α. Kidney International, 43(6): 1397-1401. https://doi.org/10.1038/ki.1993.196
[57] Shimazui, T., Nakada, T.A., Tateishi, Y., Oshima, T., Aizimu, T., Oda, S. (2019). Association between serum levels of interleukin-6 on ICU admission and subsequent outcomes in critically ill patients with acute kidney injury. BMC Nephrology, 20: 1-8. https://doi.org/10.1186/s12882-019-1265-6
[58] Mahmood, Y.S., Kathem, S.H. (2023). Protective effect of citronellol in rhabdomyolysis-induced acute kidney injury in mice. Journal of Medicine and Life, 16(7): 1057-1061. https://doi.org/10.25122/jml-2023-0102
[59] Fatima, I., Sahar, A., Tariq, A., Naz, T., Usman, M. (2024). Exploring the role of licorice and its derivatives in cell signaling pathway NF‐κB and MAPK. Journal of Nutrition and Metabolism, 2024(1): 9988167. https://doi.org/10.1155/2024/9988167
[60] Qin, M., Guo, A., Li, F., Zhang, F., Bi, M., Zhang, Y., Zhu, W. (2021). Liquiritigenin enhances cyclic adenosine monophosphate production to mitigate inflammation in dendritic cells. International Journal of Immunopathology and Pharmacology, 35. https://doi.org/10.1177/20587384211038098
[61] Yu, J.Y., Ha, J.Y., Kim, K.M., Jung, Y.S., Jung, J.C., Oh, S. (2015). Anti-inflammatory activities of licorice extract and its active compounds, glycyrrhizic acid, liquiritin and liquiritigenin, in BV2 cells and mice liver. Molecules, 20(7): 13041-13054. https://doi.org/10.3390/molecules200713041
[62] Tu, C., Ma, Y., Song, M., Yan, J., Xiao, Y., Wu, H. (2019). Liquiritigenin inhibits IL-1β-induced inflammation and cartilage matrix degradation in rat chondrocytes. European Journal of Pharmacology, 858: 172445. https://doi.org/10.1016/j.ejphar.2019.172445
[63] Zhu, X., Shi, J., Li, H. (2018). Liquiritigenin attenuates high glucose-induced mesangial matrix accumulation, oxidative stress, and inflammation by suppression of the NF-κB and NLRP3 inflammasome pathways. Biomedicine & Pharmacotherapy, 106: 976-982. https://doi.org/10.1016/j.biopha.2018.07.045
[64] Babu, V., Kapkoti, D.S., Binwal, M., Bhakuni, R.S., Shanker, K., Singh, M., Tandon, S., Mugale, M.N., Kumar, N., Bawankule, D.U. (2023). Liquiritigenin, isoliquiritigenin rich extract of glycyrrhiza glabra roots attenuates inflammation in macrophages and collagen-induced arthritis in rats. Inflammopharmacology, 31(2): 983-996. https://doi.org/10.1007/s10787-023-01152-w
[65] Wei, Z., Sun, X., He, Q., Zhao, Y., Wu, Y., Han, X., Wu, Z., Chu, X., Guan, S. (2022). Nephroprotective effect of magnesium isoglycyrrhizinate against arsenic trioxide-induced acute kidney damage in mice. Experimental and Therapeutic Medicine, 23(4): 276. https://doi.org/10.3892/etm.2022.11202