Alfian Pramudita Putra*![]() | Lolita Hapsari Dwi Syahananta
| Lolita Hapsari Dwi Syahananta![]() | Akif Rahmatillah
| Akif Rahmatillah![]() | Pujiyanto
| Pujiyanto![]() | Osmalina Nur Rahma
| Osmalina Nur Rahma![]() | I Putu Alit Pawana
| I Putu Alit Pawana![]() | Fitriyatul Qulub
| Fitriyatul Qulub![]() | Esti Andarini
| Esti Andarini![]()
© 2024 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
The patient with a spinal TB that has kyphosis will be prone to falling. Ankle Foot Orthosis (AFO) is proposed as a medical instrumentation that can help the patient's gait rehabilitation become more stable and reduce excessive leg movement. However, the design of AFO is not specified for spinal TB cases, and the fabrication process is mainly trial and error. This study aims to do a simulation based on finite element analysis on the AFO model for spinal TB patients. There were two variations in thickness (5 and 7 cm) and four types of materials (Polypropylene (PP), Carbon Fiber (CF) 230, 290, and 395) based on the available AFO used by the patient with gait disorder. The AFO model is subjected to loading according to the gait phase and cuff loading to analyze the stress, deformation, deflection, and safety factors. PP-based AFO model has the highest deformation among other materials. AFO with 7 mm thickness had lower deformation of up to half of the deformation in AFO with 5 mm thickness. The AFO model made from CF 395 at 547 MPa owns the most considerable maximum von Mises stress. In conclusion, AFO made from CF 395 with a thickness of 7 mm is considered suitable for rehabilitating spinal TB patients to provide stability. For future studies, the most suitable model of this study could be fabricated by a 3D printing process to be used by spinal TB patients.
Ankle Foot Orthosis, spinal tuberculosis, finite element analysis, rehabilitation, healthcare
Tuberculosis (TB) has become a global problem, especially in developing countries. More than 10 million people in the world suffered due to TB in 2019, with India as the highest contributor in this number (26%), followed by Indonesia in second place at 8.5% and China in third place at 8.4% [1]. Spinal TB accounts for about 50% of cases of bone TB and is a hazardous type of TB because spinal infections caused by TB bacteria can cause neurological disorders with a prevalence of 10% to 43% [2]. Even spinal TB with no longer active TB can lead to permanent spinal deformation and paraplegia [3-6]. The progressive reduction of the spine will result in the collapse of bone tissue, which causes a decrease in the mechanical strength of the bone to support body weight and causes a deformity in the form of kyphosis [4]. The formation of kyphosis can lead to a sagittal imbalance (a condition where the body can maintain an upright posture) of the body when walking so that the body will implement a compensatory mechanism characterized by knee flexion and ankle extension inducing pelvic translation. However, the existence of this compensatory mechanism makes spinal TB sufferers more prone to falling in the late stance phase [7].
Most spinal TB patients undergo medication to eradicate the bacteria, usually for six months. During this period, the patient still has to suffer from the deformation in the spine, which affects their gait. Some treatments for extrapulmonary TB sites, such as the use of orthopedic hardware, have been recommended by some experts. An extension of up to 12 months of treatment was also recommended for this case, including spinal TB [6]. The spinal deformation in spinal TB cases could lead to gait disorders. It could be treated by using orthosis, which can give more stability to the user's stature when standing and support during walking.
Ankle Foot Orthosis (AFO) is a medical instrumentation that can assist the rehabilitation process of paraplegia in spinal TB patients so that the patient's gait can approach normal conditions [8]. The type of AFO suitable for spinal TB cases is ventral AFO, which has an anterior resistance called a cuff to keep the legs balanced and sturdy enough to support body weight. To ensure the convenience of using AFO, several parameters that need to be considered in AFO design are rigidity, geometric shape, and the type of material used [9]. However, even if these parameters were as well defined as possible, for AFO whose parameters were explicitly adjusted to the situation of one patient, the probability of AFO to fracture was twice as high as for AFO whose parameter values were fixed [10]. Model design and simulation based on the Finite Element Method (FEM) are carried out with the help of computers to reduce the duration of trial and error when looking for the most optimal AFO model parameters [11].
Our previous study carried out the design and simulation of ventral AFO for cases of spinal tuberculosis [12]. The differences in safety factors from variations in the thickness of the AFO were found. The AFO model's thickness, such as the AFO's stiffness, will affect the AFO's behavior when the load is applied. Furthermore, the material choice is also essential since the AFO should maintain its mechanical integrity when walking. The Ventral AFO has a design that resembles a solid-ankle AFO that covers the posterior and inferior surfaces of the calf and foot. Still, the Ventral AFO is also equipped with a stiff anterior surface to resist excessive tibial displacement in the stance phase, increase knee stability, and provide knee torque. Extensor externally during the stance phase. This AFO is also known as ventral AFO due to the addition of the ventral part. Generally, Ventral AFO treats weakness of the plantar flexor and dorsiflexor muscles and excessive tibial shift. The design of Putra (2021) has not taken into account the influence of different materials in the AFO design and simulation [12]. In this study, the solid design of the ventral AFO model was adapted to the condition of spinal TB patients who experience spinal deformities in the form of kyphosis. The parameters varied in the AFO model, namely in terms of the material and thickness of the AFO. The simulation of the FEM numerical method was carried out to determine how the response of the variation in the AFO model to the loading simulates the gait stage during the stance phase and also loading in the cuff section. The analysis was carried out on the deformation, stress, and safety factors. The final objective of this study is to obtain a suitable and safe variation of the AFO model in rehabilitating the gait of spinal TB patients so that the gait condition can approach a normal state.
2.1 Material properties and model dimension
Four material variations were applied to the AFO model: Polypropylene (PP), 230 GPa Carbon Fiber (CF), 290 GPa CF, and 395 GPa CF. The materials are assumed to be isotropic, linear, and homogeneous. The characteristics of the materials used in the simulation can be seen in Table 1. The dimensions of the AFO model are obtained from anthropometry data of normal subjects who do not suffer from a history of spinal TB disease or spinal deformities, which represents the Indonesian population prone to have spinal TB, around the age of 21-30 [13]. The anthropometric data and body weight of the subject were presented in Table 2.
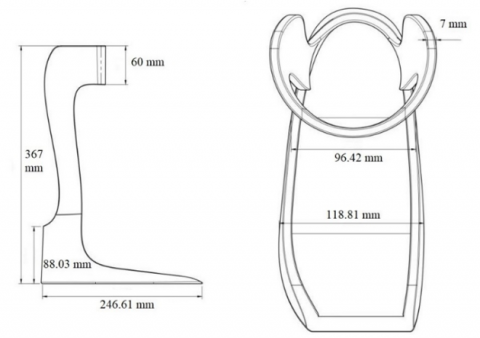
The design of the AFO model was carried out with Fusion 360 (Autodesk, Singapore). The model was built by following the current ventral AFO and using the anthropometric data of the AFO user, as stated in Table 2. AFO models have a cuff with a height of 6 cm. AFO model 1 has a thickness of 5 mm, and the AFO model 2 has 7 mm, as shown in Figures 1 and 2. The thickness used in this study was chosen based on the previous study by Gomes et al. [10], which also used 5 and 7 mm.
Table 1. The material properties used in the simulation [13-15]
|
Material Properties |
PP |
CF 230 GPa |
CF 290 GPa |
CF 395 GPa |
|
Density (kg/m3) |
902 |
1800 |
1800 |
1800 |
|
Poisson’s Ratio |
0.443 |
0.4 |
0.4 |
0.4 |
|
Young’s Modulus Y axis |
915 MPa |
230 GPa |
290 GPa |
395 GPa |
|
Young’s Modulus Z-axis |
915 MPa |
23 GPa |
23 GPa |
6 GPa |
|
Young’s Modulus X-axis |
915 MPa |
23 GPa |
23 GPa |
6 GPa |
Table 2. Anthropometric data of AFO user
|
No. |
Data |
Value |
|
1. |
Leg Height |
(36 ± 0.05) cm |
|
2. |
Foot Length |
(24 ± 0.05) cm |
|
3. |
Calf Girth |
(33.5 ± 0.05) cm |
|
4. |
Forefoot Diameter |
(7 ± 0.05) cm |
|
5. |
Malleoli Diameter |
(13 ± 0.05) cm |
|
6. |
Body Weight |
(55 ± 0.5) kg |
Figure 1. Solid model AFO 1 side view (left) and top view (right), measured in millimeters
Figure 2. Solid model AFO 2 side view (left) and top view (right), measured in millimeters
2.2 Boundary conditions settings
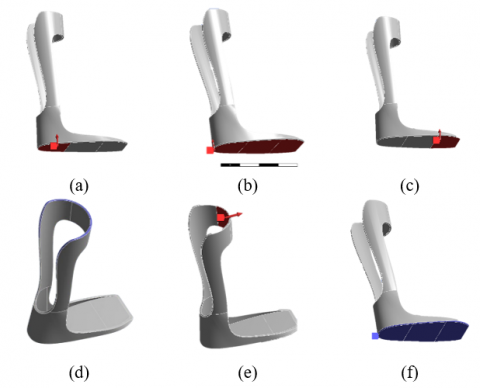
The loading points on the AFO are adjusted to represent the patient's body load on the AFO cuff and AFO footplate at the initial contact, midstance, and terminal stance stages during the gait cycle. The loading is in the same direction as the y-axis (vertical direction) and has a magnitude of 550 N for initial contact, midstance, and terminal stance. This load represents the force from the body weight of the AFO user [14]. The load on the cuff was in the x-axis direction with a magnitude of 500 N. The load occurred horizontally in the cuff since our legs moved forward while walking toward the cuff section. The load towards the cuff section is usually lower than the user’s body weight. However, in this study, we used the load near the body weight to simulate the force when the user is prone to fall forward. The previous study also used the loading condition in the gait cycle and the force towards the cuff section [12, 15, 16]. The fixed support and loading position are depicted in Figure 3.
The model was assumed to be used by the spinal TB patients, and most of the loading came from the ground reaction force, which was divided into three subphases in this study: initial contact, midstance, and terminal stance.
Figure 3. Loading area (red) and fixed support (blue) for the force on the cuff: (a) loading area in initial contact, (b) loading area in mid stance, (c) loading area in terminal stance, (d) fixed support in Ground reaction Force loading, (e) loading area in cuff loading, and (f) fixed support in cuff loading
2.3 Convergence study
Convergence studies must be conducted to determine a sufficient meshing level to obtain accurate simulation results without excessive computational burden [17, 18]. This process was performed by comparing the maximum stress value for each element size variation and taking the element size with a stable stress value as the correct element size. The mesh shape that was used in this convergence study was tetrahedral. The use of tetrahedral was based on their ease of application, which did not require further user adjustment and well-representative pressure distribution [19]. The AFO model was converged in a convergence study using the h-refinement method [20, 21]. Both AFO models converged at approximately 2.3 mm in size. For the results, von Mises stress and deformation were used to evaluate the FE model. This process also aims to validate the model to give adequate results for designing AFO for spinal TB cases.
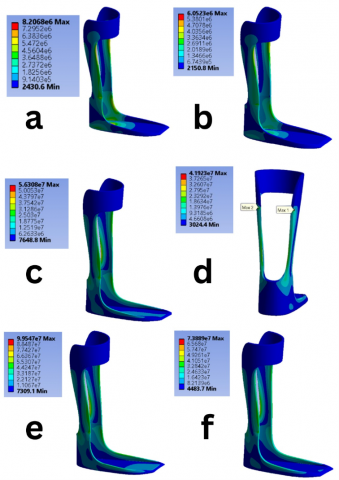
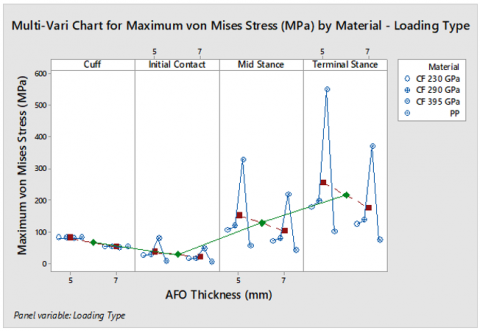
Several results of the simulation can be seen in Figure 4. The von Mises Stress result showed the stress distribution in the AFO during the stance phase. The variation of the AFO model with a thickness of 7 mm has a larger volume, so the stress distribution in the AFO model became more uniform and lowered the maximum stress. This uniform distribution is essential for the AFO model to ensure that the AFO does not receive the maximal excess stress at one point and cause it to break under the Ground Reaction Force (GRF). The maximum stress concentration point presented in the AFO model with a thickness of 5 mm is less than in the AFO model with a thickness of 7 mm, which experiences loading in the midstance phase. Thus, an AFO model with a thickness of 7 mm has fewer points that are more prone to fatigue. Figure 5 emphasizes the statement above that the maximum stress was consistently more minor in the thinner AFO. It also happens in different loading and material types. The AFO model made from CF 395 at 547 MPa owns the most considerable maximum von Mises stress.
Figure 4. The von mises stress phenogram of ankle-foot orthosis in three subphases for two different thickness modes: a. Initial Contact (5 mm), b. Initial Contact (7 mm), c. Midstance (5 mm), d. Midstance (7 mm), e. Terminal Stance (5 mm), and f. Terminal Stace (7 mm)
Figure 5. The multi-vari chart of von mises stress in terms of material type, loading types, and thickness of AFO
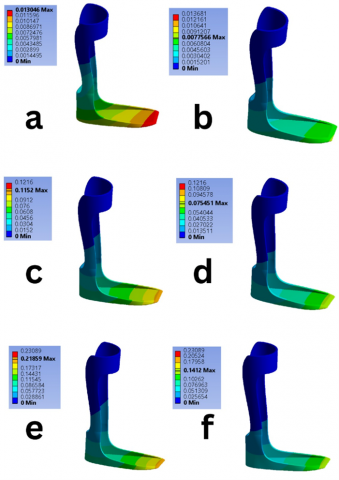
The thickness variations in the AFO model were carried out to provide rigidity to the AFO model to support the body load of spinal TB patients. The result of deformation, when loading is applied to the initial contact, midstance, and cuff loading phases, showed that increasing the thickness of the AFO model to 7 mm would result in a decrease in the deformation value of up to half of the deformation value when the thickness of the AFO model was 5 mm as shown in Figures 6 and 7. This result was aligned with the statement that adding the thickness value of the AFO model could increase its durability so that even if the same load were applied, the AFO model would not be prone to experience elongation [10, 22, 23].
Figure 6. The contour plot of deformation in ventral ankle-foot orthosis in three subphases for two different thickness modes in meter: a. Initial Contact (5 mm), b. Initial Contact (7 mm), c. Midstance (5 mm), d. Midstance (7 mm), e. Terminal Stance (5 mm), and f. Terminal Stace (7 mm)
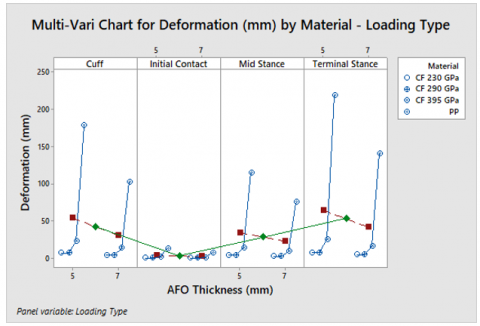
Figure 7. The multi-vari chart of deformation in terms of material type, loading types, and thickness of AFO
In some simulation results for the initial contact, midstance, and terminal stance phases, some irregularities indicate that the maximum stress is very high when fixed support is applied. This result was caused by the stress singularity arising from the simplification needed to conduct the simulation. In factual circumstances, no fixed support structure is so rigid that it does not experience movement [24]. There may be a build-up of stress at this point, but the value should not be as high as the simulation results showed. Besides, the stress singularity can be ignored because the maximum stress value was only minor compared to the overall model size.
Following the effect of thickness on stress values, the safety factor for the variation in the AFO model with a thickness of 7 mm has a higher value than the safety factor for the variation in the AFO model with a thickness of 5 mm. This result indicates that the variation of the AFO model with a thickness of 7 mm has a more remarkable ability to provide resistance to the burden of spinal TB patients and has a lower potential for fracture [25-27].
The result shows that the PP-based AFO model variations have the highest deformation among other materials during the stance phase. The difference in deformation values for variations in the AFO model material is caused by the higher elastic modulus of CF material compared to PP. Hence, the characteristics of the CF material are stiffer than the others. However, the AFO model made from CF 395 GPa had the highest modulus of elasticity among all the tested materials. It still experienced a higher deformation than CF 230 GPa and CF 290 GPa due to the modulus of elasticity in the y and z axes, which are much higher. Thus, the AFO model made from CF 395 GPa is more elastic when applied to the y and z axes.
The maximum stress received by the variation of the AFO model made of PP during the midstance, terminal stance, and cuff loading has passed the Ultimate Tensile Strength (UTS) limit of PP material, which is 29.9 MPa. Even though the variation of the PP model can still receive maximum stress in the initial contact phase, the maximum stress value is too close to the UTS value, so it will affect the fatigue speed and cause the AFO model made from PP to break faster when used routinely. This result indicates that the PP-based AFO model is not strong enough to maintain its shape while supporting the patient's body weight during the stance phase. It cannot resist abnormal knee movements in spinal TB patients. In conclusion, it is unsafe for patients to use [28, 29].
For stress analysis on the AFO model made from CF, because the UTS value for CF material is high, the stress simulation results for all variations of AFO made from CF 230 GPa, 290 GPa, and 395 GPa can still be accepted by the material without causing fractures so that the feet patient can maintain body balance during stance well. In loading the initial contact, midstance, and terminal stance phases, the most significant maximum stress value is owned by the AFO model made from CF 395. In addition, a stress singularity effect makes top stress points of very high value only appear in the fixed support section. However, on cuff loading, the maximum stress value on the AFO model made from CF 395 GPa is smaller than on other CF models made from AFO. This reason is the lower value of the shear modulus belonging to the CF 395 GPa material, which causes the maximum stress value near the trimline to experience less shear stress than other AFO models made from CF [25, 30]. The AFO CF 395 GPa model is more elastic when subjected to shear stress, providing firm support for the patient's body weight during the stance phase and flexible leg movement.
The AFO model made from PP has a maximum stress value that has passed the UTS of PP. The safety factor was the lowest among other variations of AFO materials, which meant that the AFO model made from PP was not as safe as the AFO model made from CF when used for patients because it is more prone to fracture [31]. Meanwhile, the AFO model made from CF 290 GPa, especially the AFO variation two models, has the most significant safety factor for loading the initial contact, midstance, and terminal stance phases. The AFO variation two made from CF 390 GPa has the most significant safety factor value except for the cuff loading. Even though the high safety factor value is a benchmark that the AFO model can withstand loading well, the safety factor simulation results from almost all AFO models are very high until they exceed 100%. This unrealistic safety factor value occurs because the simulation program only calculates the input value.
The Vertical Ground Reaction Force (VGRF) data will have two peaks in ordinary people who do not have a gait disorder. The first peak occurs when the gait is in the initial contact phase, where the heel hits the floor, and the center of gravity moves closer to the floor surface, causing an increase in the floor's reaction force in the vertical direction. Meanwhile, the second peak occurs in response to the floor's response to the force generated by the plantar flexion in the terminal stance just before toe-off to move the body forward [32]. On the other hand, the balance compensation mechanism in spinal TB patients, which affects the appearance of dorsiflexion during the stance phase, causes the thrust against the body to be less than usual, so the second peak in VGRF decreases [33].
The condition causes the legs of spinal TB patients to become unstable in supporting the body and makes them prone to falling in the final terminal stance phase. This condition is where the ventral AFO plays a role in reducing ankle extension, which will lead to the prevention of excess tibial movement so that the VGRF of spinal TB patients in the terminal stance phase can reach a value sufficient to produce near-normal gait [3, 34, 35]. Based on the maximum stress value data obtained from the simulation, the AFO model experiences the highest maximum stress in the terminal stance phase and then in the initial contact phase. Peak stress values in these two phases indicate that the AFO model increases VGRF in the terminal stance phase, stabilizing spinal TB patients' gait [36].
The AFO variation two models made from CF 395 GPa are considered the most suitable for use by patients with spinal tuberculosis because of their mechanical characteristics that are strong enough to provide a knee extensor moment externally and are elastic enough to allow regular gait movements to suit the needs of spinal TB patients. The impact of using this AFO configuration in the clinical setting is that the patient will have a more rigid ankle since the material is stiff, and the stress distribution result showed a high safety factor. In addition, the stability of the user will be maintained.
Several limitations were present in this study. First, the AFO model is only a rigid body that uses isotropic and homogenous materials. The model itself did not have a fixator to the foot, like straps on the calf or foot. The use of fixed support as the boundary condition in the model aimed to mimic the role of supporting items in the AFO. Further study in finite element analysis using more than a single rigid body is needed to analyze the model's response to a more realistic model, such as straps and foot models. However, the result of this study already showed that the effect of materials and thickness in the AFO model could give information about the crucial location in which the pressure is located, and it is acceptable. More complex analysis is needed to obtain a more realistic result.
The other limitation is the applied load in the model. The load related to the body weight was involved in the sole area based on their subphase in the gait cycle. Three subphases were used in this study. The common subphase is in which a pressurized area is located. That is why the loading simulation is modeled in static conditions. However, it is better to simulate the full version of loading behavior in the stance phase as a cycle to mimic walking conditions. The result of this study in three different subphases indicated that the highest von Mises stress was found in the initial contact subphase. Initial contact is an essential subphase in the gait cycle since it is the point where the foot comes into contact with the floor, and it should maintain the body weight along with the stance phase. The simulation is patient-specific because the loading condition is related to body weight. The AFO model itself is customizable and different for each user.
The varied dimensions and types of AFO materials affect the results of deformation and stress, which lead to different safety factor values for each variation of the AFO model. In this simulation, the variation of the AFO model made from PP with a thickness of 7 mm has a higher safety factor than the variation in the AFO model made from CF with a thickness of 5 mm. The high-value safety factor indicates that AFO has sufficient ability to accept stress from gait cycle loading. The AFO considered suitable for rehabilitating spinal TB patients is the AFO variation two models made from CF 395 GPa with a thickness of 7 mm. By having this result, a more dedicated AFO for spinal TB patients could be optimized. It can be an optional rehabilitation strategy for spinal TB cases that undergo a medication procedure of tuberculosis drugs. The future study could apply a loading to the AFO model using dynamic loading based on the ground reaction force data of spinal TB patients and test the effect of the AFO model on the gait of spinal TB patients directly. In addition, the high safety factor value of the AFO carbon fiber model can be overcome by reducing the value in dimensional variations, which can make the fabrication process of the AFO model made from carbon fiber easier. The design should be fabricated and validated using an experimental set-up indicating the condition of spinal TB patients for further implementation.
We express our profound gratitude to the Faculty of Science and Technology at Universitas Airlangga, Indonesia, for their generous financial support of our work. This research was funded by the Novice Lecturer Research Grant for the year 2023 (Grant No.: 1898/UN3.1.8/PT/2023).
[1] World Health Organization. (2020). Global Tuberculosis Report 2020. Geneva: World Health Organization.
[2] Rasouli, M.R., Mirkoohi, M., Vaccaro, A.R., Yarandi, K.K., Rahimi-Movaghar, V. (2012). Spinal tuberculosis: Diagnosis and management. Asian Spine Journal, 6(4): 294-308. https://doi.org/10.4184/asj.2012.6.4.294
[3] Garg, R.K., Somvanshi, D.S. (2011). Spinal tuberculosis: A review. The Journal of Spinal Cord Medicine, 34(5): 440-454. https://doi.org/10.1179/2045772311Y.0000000023
[4] Jain, A.K., Kumar, J. (2013). Tuberculosis of the spine: Neurological deficit. European Spine Journal, 22(Suppl 4): 624-633. https://doi.org/10.1007/s00586-012-2335-7
[5] Pandita, A., Madhuripan, N., Pandita, S., Hurtado, R.M. (2020). Challenges and controversies in the treatment of spinal tuberculosis. Journal of Clinical Tuberculosis and Other Mycobacterial Diseases, 19: 100151. https://doi.org/10.1016/j.jctube.2020.100151
[6] Soeroso, N.N., Pradana, A., Lubis, N., Soeroso, L. (2018). Successful treatment of total paraplegic patient due to tuberculous spondylitis. Respirology Case Reports, 6(6): e00333. https://doi.org/https://doi.org/10.1002/rcr2.333
[7] Barrey, C., Roussouly, P., Le Huec, J.C., D’Acunzi, G., Perrin, G. (2013). Compensatory mechanisms contribute to keeping the sagittal balance of the spine. European Spine Journal, 22(Suppl 6): S834-S841. https://doi.org/10.1007/s00586-013-3030-z
[8] Feng, Y., Song, Y. (2017). The categories of AFO and its effect on patients with foot impair: A systemic review. Physical Activity and Health, 1(1): 8-16. https://doi.org/10.5334/paah.3
[9] Surmen, H.K., Akalan, N.E., Arslan, Y.Z. (2018). Design, Manufacture, and Selection of Ankle-Foot Orthoses. In Encyclopedia of Information Science and Technology, Fourth Edition. https://doi.org/10.4018/978-1-5225-2255-3.ch027
[10] Gomes, G., Lourenço, I., Oliveira, J., Gomes, M., Vale, A., Freire, L., Quental, P., Policarpo, H., Matos, J. (2017). Structural Reinforcements on AFO’s: A study using Computer-Aided Design and finite element method. In IEEE 5th Portuguese Meeting on Bioengineering (ENBENG), Porto, Portugal, pp. 1-4. https://doi.org/10.1109/ENBENG.2017.7889432
[11] Marques, M.A., Mendes, E., Ramos, N.V, Pinto, V.C., Vaz, M.A. (2010). Finite element analysis of ankle-foot orthosis to predict fracture conditions during gait Finite-element analysis of ankle-foot orthosis to predict fracture conditions during gait. 1st ICH Gaia-Porto.
[12] Putra, A.P., Rahmatillah, A., Pujiyanto, Ain, K., Rodiyah, N.K., Pawana, I.P.A., Syahananta, L.H.D., Dwiatma, M.R., Hidayat, A.S. (2021). Computational study of ventral ankle-foot orthoses during stance phase for post-surgery spinal tuberculosis rehabilitation. In: Triwiyanto, Nugroho H.A., Rizal A., Caesarendra W. (eds) Proceedings of the 1st International Conference on Electronics, Biomedical Engineering, and Health Informatics. Lecture Notes in Electrical Engineering, Springer, Singapore, vol. 746. https://doi.org/10.1007/978-981-33-6926-9_38
[13] Garg, B., Mehta, N., Mukherjee, R.N., Swamy, A.M., Siamwala, B.S., Malik, G. (2022). Epidemiological Insights from 1,652 patients with spinal tuberculosis managed at a single center: A retrospective review of 5-year data. Asian Spine Journal, 16(2): 162-172. https://doi.org/10.31616/asj.2021.0137
[14] Ramlee, M.H., Kadir, M.R., Murali, M.R., Kamarul, T. (2014). Biomechanical evaluation of two commonly used external fixators in the treatment of open subtalar dislocation—A finite element analysis. Medical Engineering & Physics. 2014, 36(10): 1358-1366. https://doi.org/10.1016/j.medengphy.2014.07.001
[15] Faustini, M.C., Neptune, R.R., Crawford, R.H., Stanhope, S.J. (2008). Manufacture of passive dynamic ankle-foot orthoses using selective laser sintering. IEEE Transaction in Biomedical Engineering, 55(2 Pt 1): 784-90. https://doi.org/10.1109/TBME.2007.912638
[16] Mircea, B., Carmen, P., Delia, B. (2013). Ankle foot orthoses with wire insertion. Applied Mechanics and Materials, 371: 554-558. https://doi.org/10.4028/www.scientific.net/AMM.371.554
[17] Patil, H., Jeyakarthikeyan, P.V. (2018). Mesh convergence study and estimation of discretization error of hub in clutch disc with integration of ANSYS, IOP Conference Series: Materials Science and Engineering, 402(1): 012065. https://doi.org/10.1088/1757-899X/402/1/012065
[18] Trott, D.W., Gobbert, M.K. (2010). Conducting finite element convergence studies using COMSOL 4.0. In Proceedings of the COMSOL Conference 2010 Boston, pp. 1-6.
[19] Ruggiero, A., D’Amato, R., Affatato, S. (2019). Comparison of meshing strategies in THR finite element modelling. Materials, 12(14): 1-11. https://doi.org/10.3390/ma12142332
[20] Roarty, C.M., Grosland, N.M. (2004). Adaptive meshing technique applied to an orthopaedic finite element contact problem. Iowa Orthopedic Journal, 24: 21-9.
[21] Ramlee, M.H., Sulong, M.A., Garcia-Nieto, E., Penaranda, D.A., Felip, A.R., Kadir, M.R.A. (2018). Biomechanical features of six design of the delta external fixator for treating Pilon fracture: A finite element study. Medical & Biological Engineering & Computing, 56(10): 1925-1938. https://doi.org/10.1007/s11517-018-1830-3
[22] Ielapi, A., Forward, M., De Beule, M. (2019). Computational and experimental evaluation of the mechanical properties of ankle-foot orthoses: A literature review. Prosthetics, and Orthotics International, 43(3): 339-348. https://doi.org/10.1177/0309364618824452
[23] Wojciechowski, E., Chang, A.Y., Balassone, D., Ford, J., Cheng, T.L., Little, D., Menezes, M.P., Hogan, S., Burns, J. (2019). Feasibility of designing, manufacturing and delivering 3D printed ankle-foot orthoses: A systematic review. Journal of Foot and Ankle Research, 6(11): 1-12. https://doi.org/10.1186/s13047-019-0321-6
[24] Bi, Z. (2018). Finite Element Analysis Applications: A Systematic and Practical Approach. Missouri: Elsevier. https://doi.org/10.1016/C2016-0-00054-2
[25] Eddison, N., Mulholland, M., Chockalingam, N. (2017). Do research papers provide enough information on design and material used in ankle-foot orthoses for children with cerebral palsy? A systematic review. Journal of Children’s Orthopaedics, 11(4): 263-271. https://doi.org/10.1302/1863-2548.11.160256
[26] Pourhosseingholi, E., Farahmand, B., Bagheri, A., Kamali, M., Saeb, M. (2019). Efficacy of different techniques of AFO construction for hemiplegia patients: A systematic review. Medical Journal of the Islamic Republic of Iran, 33: 50. https://doi.org/10.34171/mjiri.33.50
[27] Totah, D., Kovalenko, I., Saez, M., Barton, K. (2017). Manufacturing choices for ankle-foot orthoses: A multi-objective optimization. Procedia CIRP, 65: 145-150. https://doi.org/10.1016/j.procir.2017.04.014
[28] Bregman, D.J.J., De Groot, V., Van Diggele, P., Meulman, H., Houdijk, H., Harlaar, J. (2010). Polypropylene ankle-foot orthoses to overcome drop-foot gait in central neurological patients: A mechanical and functional evaluation. Prosthetics and Orthotics International, 34(3): 293-304. https://doi.org/10.3109/03093646.2010.495969
[29] Ramsey, J.A. (2011). Development of a method for fabricating polypropylene non-articulated dorsiflexion assist ankle-foot orthoses with predetermined stiffness. Prosthetics, and Orthotics International, 35(1): 55-69. https://doi.org/10.1177/0309364610394477
[30] Ross, R.S., Greig, R.J., Convery, P. (1999). Comparison of bending stiffness of six different colours of copolymer polypropylene. Prosthetics, and Orthotics International, 23(1): 63-71. https://doi.org/10.3109/03093649909071613
[31] Gijon-Nogueron, G., Palomo-Toucedo, I., Gil-Tinoco, A., Ortega-Avila, A.B., Munuera-Martínez, P.V. (2018). The effect produced on ground reaction forces by a prefabricated, weight-bearing and non-weight-bearing foot orthosis in the treatment of pronated foot: Pilot study. Medicine, 97(22): e10960. https://doi.org/10.1097/MD.0000000000010960
[32] Makaram, N., Arnold, G., Wang, W., Campbell, D., Gibbs, S., Abboud, R. (2016). Does the ankle-foot orthosis improve vertical forces during gait in children with spastic diplegic cerebral palsy? A retrospective 3-D gait analysis of 19 children. Orthopaedic Proceedings, 98-B(SUPP_12): 11. https://doi.org/10.1302/1358-992X.98BSUPP_12.SCOT2016-011
[33] Meadows, B., Bowers, R., Owen, E. (2008). Biomechanics of the Hip, Knee, and Ankle (4th ed.). In J. Michael, J. Hsu, and J. Fisk, eds., AAOS Atlas of Orthoses and Assistive Devices, Philadelphia.
[34] Daryabor, A., Arazpour, M., Sharifi, G., Bani, M.A., Aboutorabi, A., Golchin, N. (2017). Gait and energy consumption in adolescent idiopathic scoliosis: A literature review. Annals of Physical and Rehabilitation Medicine, 60(2): 107-116. https://doi.org/10.1016/j.rehab.2016.10.008
[35] Haddas, R., Belanger, T. (2017). Clinical gait analysis on a patient undergoing surgical correction of kyphosis from severe ankylosing spondylitis. International Journal of Spine Surgery, 11(3): 18. https://doi.org/10.14444/4018
[36] Putra, A.P., Hidayat, A.S., Rahmatillah, A., Pujiyanto, Ain, K., Pawana, I.P.A., Gusti, A.W.R. (2023). Influence of retromalleolar trimline dimensions on posterior leaf spring ankle-foot orthosis stiffness: A finite element analysis approach. Mathematical Modelling of Engineering Problems, 10(3): 979-984. https://doi.org/10.18280/mmep.100331