Fara Randrianarivelo | Adel Badri* | François Gauthier | Bryan Boudreau-Trudel |
© 2022 IIETA. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
Unlike workplace accidents, occupational diseases are often underestimated and underreported since their effects appear gradually over time. They are even on the increase in the province of Quebec (Canada), especially in small and medium-sized enterprises (SMEs), where they are less likely to receive medical attention. The aim of this four-stage study is therefore to describe how prevention of occupational disease is practiced in this type of business and identify a way forward to improve the protection of worker health and well-being in Quebec. The present article focuses on the first two stages, namely reviewing the literature to catalog the elements of prevention and identifying the most relevant elements. Stages 3 and 4, in which gathered field data on the application of these elements and analyzed their relative effectiveness using descriptive statistics, are reported in Part 2 [1]. Despite the limitations of this research method, we portray in detail the elements that appear to have the most influence on occupational disease prevention in small to medium-sized manufacturing enterprises, and thus identify the strengths and weaknesses of occupational health and safety performance in this setting.
management, manufacturing, occupational health and safety (OHS), occupational disease, prevention, small and medium-sized enterprises (SMEs), workplace accident
A small and medium-sized enterprise (SME) is defined generally as having annual sales limited to a regional market [1]. Definitions vary from one country to the next [2]. Mahé De Boislandelle [3] used four characteristics: size (10 to 500 employees), activity (specificity), ownership structure, mode of administration. Independence, that is, not being a subsidiary of a large corporation, was added later [4].
In the province of Quebec (Canada), this category of business is defined as a company staffed with not more than 499 employees and declaring annual sales of less than $50 million [5]. In fact, 72% of Quebec businesses in this category employ fewer than 10 persons, and 51% employ fewer than 5 persons. Only 2% staff 100 to 500 employees [6]. Besides size, annual sales and independence, certain other characteristics, including how occupational health and safety (OHS) is also managed distinguish SMEs.
Since 98% of all registered businesses in Quebec are SMEs, the success of this category is a major indicator of economic prosperity in the province, contributing 50% of the gross domestic product and employing 67% of the labor force [7, 8]. Their predominance in all industrial sectors favors employability and job creation [8, 9].
The human and social costs of occupational diseases is felt throughout society. Absenteeism for health reasons implies not only losses of business productivity but also medical costs, administrative costs and ultimately makes a nation less competitive for investment capital [10]. The average annual cost of occupational diseases in Quebec reached $\$$4.84 billion during the years 2010 to 2012, and the average cost of an occupational disease reached $\$$211,600, about five times as much as the average cost of a workplace accident [11]. These authors found that harm resulting from exposure to noise was the single largest cost, at $\$$777 million. During the period of 2007 to 2012, hearing and musculoskeletal diseases were the most frequent causes of claims for compensation.
The principal occupation-related cause of death in Quebec is cancer. During the period of 2002 to 2006, about 8% of all fatal cancers (1070 to 1700 per year) were attributed to exposures in the workplace. The symptoms often did not become apparent until after decades of exposure [12].
In summary, occupational diseases increased steadily by 2.7% per year during the period of 2007 to 2012, while workplace accidents decreased steadily (-4.8% per year) over the same period [13]. The number of deaths due to occupational disease has been consistently higher than the number caused by workplace accidents [14].
Accident prevention plays a major role in the viability of SMEs [15]. However, OHS status is often more precarious in this setting than in large corporations [8, 16]. In fact, occupational lesions or diseases are about eight times more frequent in the SMEs workplace [17-19].
Here, we summarize how occupational ailment prevention is practiced in Quebec SMEs, by identifying the various means implemented in this setting, based on a review of the literature. The overall aim of this study, reported in a series of two articles, is to orient future research, if not practice in the workplace, towards better protection of the health of workers in Quebec. Following this introduction, the research methodology is described in section 2, the results of the bibliographic search are presented and discussed in section 3, and a conclusion is provided in section 4.
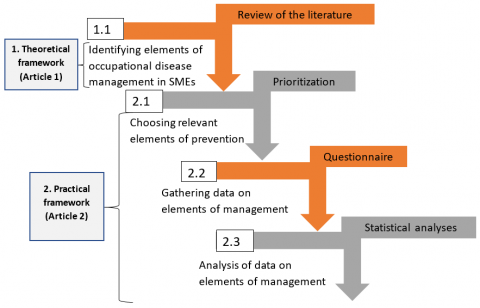
The method by which we identified elements that could be integrated advantageously into the practice of preventing occupational diseases in SMEs in Quebec was essentially a review of the literature retrieved using appropriate keywords. The practical application of these elements is the subject of the second article [1]. The theoretical framework of the overall study thus consists of three steps: 1) identifying the means that are implemented to prevent occupational diseases; 2) gathering data on how implementation is supposed to occur in specific industrial settings, and 3) analyzing actual practice to identify deficiencies and obstacles to implementation in SMEs. Recommendations to guide future research are then formulated. The methodological framework of the research and hence of the two articles in which its findings are reported is illustrated in Figure 1.
Figure 1. Methodological structure of the overall study (parts 1 and 2)
It should be noted that in this study, “elements of management” refer to variables or factors that allow practitioners to influence the effectiveness of occupational disease prevention measures. The “practice” of elements of management refers to how the SME overall applies or complies with these elements.
2.1 Identification of elements of occupational disease prevention
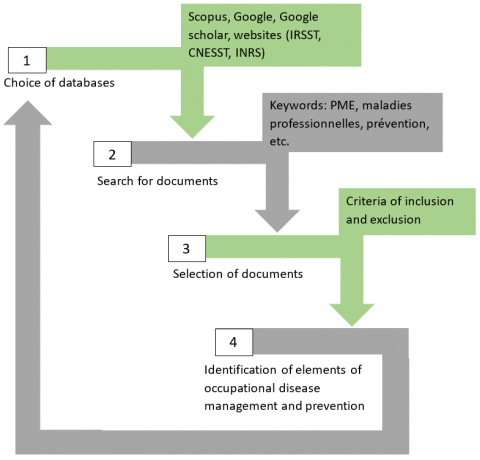
The literature was searched using the database Scopus, the search engines Google and Google Scholar, the websites of the Institut de recherche Robert-Sauvé en santé et en sécurité du travail (IRSST), the Commission des normes, de l’équité, de la santé et de la sécurité du travail (CNESST) and Institut national de recherche et de sécurité (INRS).
Keywords in English and French were used: "OHS', 'OHS performance", "OHS management", "occupational disease", SME, "prevention of occupational diseases", "management of occupational diseases in SMEs", "elements of OSH management", "characteristics of SMEs", and "occupational risk management".
It should be noted that this bibliographic research methodology is a hybrid and not systematic. The reason for this orientation is that the research targets a particular place and sector where technical documentation is dominant. This documentation is of paramount importance for this research.
Documents retrieved included articles published in scientific journals, conference proceedings, research reports, theses, memoirs, standards, regulations, and legislation. In order not to overlook important elements of occupational disease management and prevention, research on businesses of all sizes was considered. Documents on public health were not included.
Numerous elements of prevention management were thus identified. Some of these were not specific for occupational disease. However, they may be relevant to OHS management in general.
Figure 2 summarizes the steps involved in identifying the elements of occupational disease management and prevention.
Figure 2. Identifying elements of occupational disease management and prevention
3.1 Concept of occupational health and safety performance
OHS performance is defined differently by different authors Liu et al. [20]. Dı́az and Cabrera [21] refer to "safe behavior of employees aware of the hazards in their work environment". Wu et al. [22] associate OHS performance with the robustness of the OHS management system in place. An objective measurement of performance would be the frequency of occupational disease in a business, per year per given number of employees [23]. Another measurement would be the length of time over which a company was free of accidents and diseases [24]. In any case, performance is a measurement of the effectiveness of the OHS management in place, especially where occupational diseases have been reduced or eliminated on the short or medium term [17].
Several elements may reflect OHS performance, such as the number of activities relating to prevention, the number of workers involved in or benefitting from these activities, the level of exposure to hazards [25], the incidence and seriousness of lesions, and the dollar value of approved claims for compensation [26].
The three main approaches to measuring OHS performance are: 1) analysis of results, 2) auditing of compliance, and 3) auditing of processes [27]. The two types of performance indicators are reactive and proactive [28, 29]. These are complementary and should be used conjointly [17, 30]. Results-based performance measurement uses reactive indicators, which are based on historical data, that is, harmful events that have already occurred [29, 31, 32]. Proactive indicators are focused on compliance with preventive measures designed to prevent lesions from occurring in the workplace [29]. However, the number of injuries and deaths may be cited [28]. Ten proactive indicators that have gained widespread acceptance [33] for OHS performance evaluation are: 1) accountability, 2) communication and consultation, 3) involvement of employees, 4) involvement of managers, 5) feedback on and recognition of involvement, 6) prevalence of awareness, 7) risk management, 8) management systems, 9) inspections, and 10) workplace practice (training offered, information disseminated, interventions, tools and resources used).
3.2 Elements influencing OHS performance
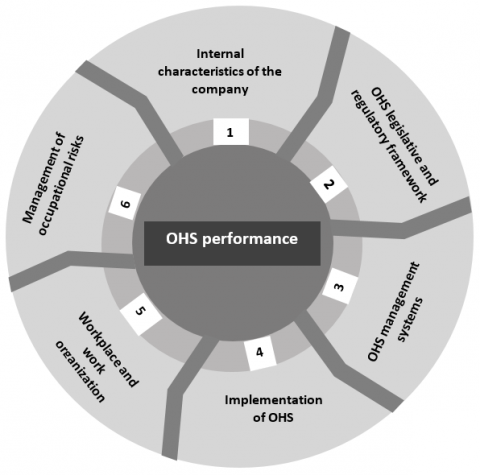
Numerous elements influencing OHS performance in SMEs are mentioned repeatedly in the literature. In this study, these have been grouped into six families (Figure 3), as follows: 1) Internal characteristics of the company [26, 34-36], 2) OHS legislative and regulatory framework [37], 3) OHS management systems, 4) Implementation of OHS [26], 5) Workplace and work organization [26], and 6) management of occupational risks [17, 33].
Figure 3. The six families of elements that influence OHS performance
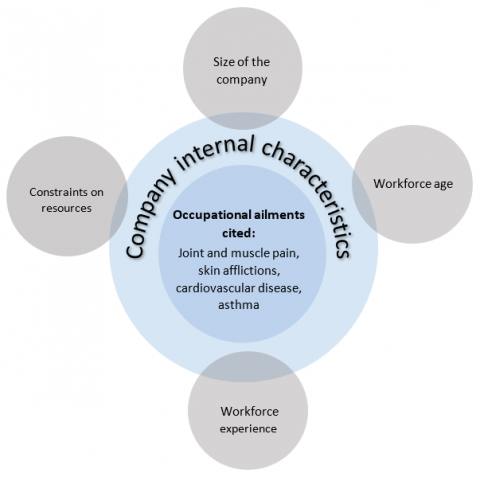
3.2.1 Internal characteristics of the company
Interest in OHS appears to decrease with the size of the company [38]. Worker age, gender, and work experience [36, 26] and constraints on resources [8, 16, 26, 39, 40] all affect OHS performance in SMEs directly.
Size of the company. OHS performance is poorer in small companies than in large companies [8, 16, 41, 42]. Company smallness is an element that favors occupational lesions [41], and workers in SMEs suffer work-related harm more often than those employed by large corporations [43, 44]. As company size increases, OHS management activities seem to improve [45], evaluations become more frequent [46], and implementation of preventive measures increases [47]. Training paid by the employer also is proportional to company size [48]. Training specifically for OHS has a positive influence on worker behaviors and attitudes towards health and safety [49]. Among specific risk factors that have been found to increase as company size decreases are musculoskeletal diseases [50] and exposure to solvents [51]. All organic solvents are potentially harmful to human health, causing skin afflictions (irritation, burns and dermatoses) and disorders associated with the nervous system (dizziness, impairment, paralysis, etc.), blood (anemia), liver (hepatitis) and kidneys [52].
Workforce age. In general, younger workers take on more physically demanding and risky tasks [53, 54]. They often accept employment in manufacturing, where they are exposed to numerous dangerous substances. The risk of work-related skin diseases is greater among young employees. Joint and muscle pains associated with repetitive movements and handling heavy loads are also more frequent [55]. In fact, it has been known for decades that injury in the workplace is more frequent among younger workers [56]. Younger workers are also generally more exposed to vibrations from equiSMEnt and tools [55] and are very sensitive to hazardous substances.
As workers age, their physical capacities (load bearing, endurance, strength, visual acuity) and their cognitive capacities decrease [53, 54]. Older workers often push themselves beyond their capacities, to maintain their overall performance [57], leading to a variety of occupational diseases including joint and muscle injury [58], which is often age-related [59, 60]. The proportion of individuals living with at least two of the 10 most common chronic afflictions (hypertension, coronaropathy, stroke, diabetes, cancer, arthritis, hepatitis, kidney failure, lung disease, asthma) increases with age [61]. Older workers regularly suffer from heart disease and sleep disorders [62].
Workforce experience. Workers with more experience and seniority have fewer recent work-related diseases or risk of injury [63]. Several studies have shown that the more experience a worker acquires, the more strategies he develops to protect himself against risks and manage physical challenges on the job [64-66]. Experience could be contributing to know-how that reduces the risk of joint and muscular problems [67]. Work-related manual skill and dexterity tend to increase with years on the job [68]. Furthermore, workplace accidents occur more frequently in association with unusual tasks [69]. For all these reasons, new employees are more inclined to suffer occupational injuries and lesions.
Gender. A given task may be physically more onerous for women [70], since they are on average smaller than men and frequently have lower muscle strength and aerobic capacity. Women possess on average about two-thirds the physical strength of men, which creates a gender-based differential in load-handling capacity [71]. Some studies suggest that joint and muscle diseases are generally more common in women [72], depending on the type of ailment [73]. Women tend to suffer more from diseases of the upper limbs [74] and the neck [75]. This may be due to performing more repetitive manual tasks requiring precision [55]. Textile workers are more often women, which exposes them more to fibrous dust [76]. The personal protection devices that they use are often not properly designed for or adjustable to female faces and bodies [77-79]. This can increase the risk of inhalation and skin contact with chemicals and noxious particles, and the risk of falls, among others [77].
In general, men are more subjected than women to physical constraints in the workplace [80] and as a result suffer more knee pain [75]. Men are also more exposed overall to noise, since they make up most of the labor force in mines, on construction sites, in heavy manufacturing and so on [81]. Exposure to noise in the workplace can lead to hearing loss and is a major risk factor for cardiovascular disease [82, 83]. In Québec, work-related deafness is more common among men than women [84].
It has been found that men eliminate chemicals from their system faster than women do [85]. The faster the body can eliminate chemical toxins, the lower is the risk of developing the associated occupational disease [86].
Constraints on resources. Scarcity of key resources (economic, human, technological) opposes obstacles to the improvement of OHS in SMEs [8, 16, 26, 40, 87, 88]. For 63% of SMEs in Quebec, annual sales do not exceed $500,000 [6]. The costs of implementing preventive measures can be prohibitive in such businesses [89] and OHS therefore tends to stay on the back burner [90]. Even compliance with OHS regulation can be unrealistic [16]. It therefore comes as no surprise that the same applies to OHS training in SMEs [35]. The current offerings by firms specialized in OHS training are often considered too technical and too expensive [89]. Regarding support for prevention, the provincial OHS standards and equity board (CNESST) has been focused more on large corporations than on SMEs and promoting OHS in the SME sector has been under-budgeted and underfunded [91]. The elements that influence OHS performance are summarized in Figure 4.
Figure 4. Summary of the elements that influence OHS performance in businesses
3.2.2 OHS legislative and regulatory framework
The legislative and regulatory framework for preventive measures in the workplace in Quebec consists of the occupational health and safety act (LSST) and occupational health and safety regulations (RSST).
The aim of the LSST is to formalize the obligation to eliminate health and safety hazards and threats to the physical integrity of workers at the source (LSST, article 2). To achieve this goal, prevention is presumed to be undertaken by committees in the workplace, on which workers, managers and employers participate jointly. The act sets forth the responsibilities of employers (article 49) and those of workers (article 51) regarding the prevention of workplace accidents and occupational diseases or diseases.
Regulations are derived from the text of the act. They specify certain requirements regarding OHS, covering among others proper architecture and furnishing of the work environment, standards for machinery and equiSMEnt, specific working conditions (closed spaces, heights, etc.) and collective as well as personal means of protection [92, 93].
The various regulatory requirements for OHS are not as binding for SMEs [8, 19, 94, 95]. Inspections by firms specialized in OHS are oriented more towards large corporations and the most dangerous industrial sectors [38, 96]. Compliance of SMEs with OHS regulations is difficult [97] and generally limited to the strict minimum necessary to avoid infractions against CNESST code [98]. This does not go without creating tensions and conflict within these companies. Some managers of SMEs are critical of OHS legislation, feeling that the concept of OHS is poorly adapted to SME reality [98]. Managers and workers are often aware of OHS standards and regulations but find them too difficult or impractical to apply.
The LSST recognizes three mechanisms or means (interventions) of prevention: health and safety committee, prevention program (which includes the health program) and the prevention representative.
The health and safety committee. The committee is an in-house and joint participation mechanism of implementing OHS. SMEs in priority groups I and II, having more than 20 employees are obliged to form such a committee (LSST, article 68). However, if need be, the CNESST can require any company, regardless of size, to form a health and safety committee (LSST, article 69). Even in the absence of obligations, managers of SMEs often set up a committee after a major safety or health event has taken place in the company. Constitution of OHS committees in SMEs is subject to cultural and economic factors [99]. A certain company size and employee unionization are often preconditions for setting up a health and safety committee [94].
Several functions are associated with the HS committee. It is set up initially to identify potential health and safety issues in the company and raise awareness among workers, managers, and employers [100]. Proactive approaches begin by exploring working conditions. A preventive action plan is then developed, and activities are arranged. The committee also ensures that the prevention policy is spread by all workers, monitors the effectiveness of the actions, and anticipates adjustments that might become necessary [101]. Its existence makes it possible to formulate recommendations, support prevention activities, and evaluate and improve the management of prevention [102]. It participates in the choosing of the most appropriate personal protective devices for the activities of the company, validates the prevention program and names a physician as overseer of on-site health services. It is also involved in the identification and evaluation of health and safety risks and develops training programs and information for the purposes of prevention (LSST, art.178).
The success of the health and safety committee depends mainly on the work climate prevailing in the company, specifically how much this garners the support and involvement of the workers. The committee has been described as one of the most important means of getting workers to participate in prevention [103]. Worker involvement favors prevention [104, 105], even though workers tend not to support this approach [106]. Support by the company directors [107], especially visible attention to committee recommendations [100] influences effectiveness and accelerates implementation [108]. However, decision-making must be rapid; members must be willing to compromise, genuinely interested in the results, and trusting of one another [104]. This requires that they understand how the committee is supposed to work [104, 107, 109]. The frequency of meetings, the agenda, decorum and protocol, mandates and leadership roles must be clear and understood [104, 107]. The recommendations must not be overwhelming in number or perceived as onerous to implement and must be accepted as helpful by a majority [107].
The prevention program. This program is a single document listing the strategic activities devised specifically for the company to bring under control or eliminate occupational hazards and OHS risks [110]. It is required (LSST, art. 4) for SMEs in the first three top priority categories (having more than 20 employees) and is tailored to the needs of the company [111].
The purpose of the program is to harmonize the activities, allow their improvement and promote a culture of prevention within the company. It describes the company health program, adaptation to the standards set by regulation, measures for monitoring the quality of working conditions and preventive maintenance, standards of safety and hygiene, required means or devices for individual protection, and lists the OHS training programs and information sessions planned. Managers of SMEs generally find the production of this program onerous, and the guidelines complicated [94]. Most of these businesses turn to firms specialized in the production of the required document. Workers may be consulted at this stage, since the workplace and the tasks performed therein must be examined systematically and past events analyzed [112]. OHS risks are thus identified, but at a considerable cost.
The success of the prevention program depends initially on commitment and support from upper management [111] and then on the accuracy of the risk factor analysis and the realism of the plan of action [112]. However, success depends ultimately on how well the workers take up knowledge of OHS risks and how much they comply with the safety procedures written in the program [111].
The prevention representative. A worker must be designated to assume certain responsibilities set forth in the prevention program. When the company has a health and safety committee, this worker is automatically a member and representative of the program. SMEs with more than 20 employees must designate such a representative (RSST, art.1), as must any company that has an HS committee, regardless of size (LSST, art. 87).
The tasks of the representative revolve around reducing workplace accidents. He/she assists the CNESST inspector during visits by the latter in the company and is also involved when a worker asserts his/her right of refusal (LSST, art. 90). The representative participates in all scheduled prevention activities, as do all HS committee members. The employer is required to cooperate with the prevention representative and must provide him/her with all materials needed for the completion of his/her tasks (RSST, art. 6).
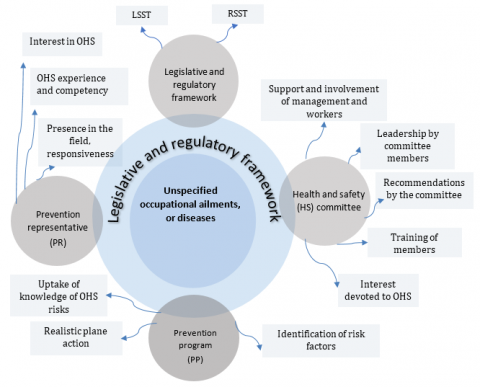
The success of the representative’s efforts depends on support by and involvement of management as well as his/her interest in OHS. His/her collaboration with the HS committee, listening skills, presence in the field and responsiveness all favor success. The person also must have relevant OHS experience and competency. The elements of OHS performance associated with the legislative and regulatory framework are summarized in Figure 5.
Figure 5. Summary of the elements of OHS performance associated with the legislative and regulatory framework
3.2.3 OHS management systems
An occupational health and safety management system (OHSMS) is a means of monitoring and intervention adapted to the size and production activities of the business. It is a fundamental element of the overall management of the company [113], dedicated to the analysis and management of risks [114]. An OHSMS must facilitate, not hinder, the prevention-related tasks of managers [115]. Its application must be systematic, and improvements in OHS performance should occur accordingly. Employers can use it to change attitudes towards occupational risks, maintain correct attitudes [116], consolidate the company brand image and compliance with OHS regulation and improve work conditions as well as internal communication [113].
The three most widely used OHS management references are the Occupational Health and Safety Assessment Series (OHSAS 18001) produced by the British Standards Institute (BSI), Canadian Standards Association standard Z1000 [117] and ISO standard 45001 [118]. In addition, the International Labor Organization proposes guiding principles in ILO-OSH 2001 [117]. An OHSMS based solidly on any of these references is more likely to succeed.
Implementation of an OHSMS is generally challenging. Competency and technical knowledge as well as financial means beyond those of most SMEs are required [114, 119]. However, some of the steps can be made easier by integrating specific training programs [114] such as WISE (Work Improvement in Small Enterprises) or WIND (Work Improvement in Neighborhood DeveloSMEnt). Some specific requirements have been set for SMEs [120]: 1) implementation of a written safety policy, 2) analysis of risks (production processes, circulation, handling, storage, and transport), 3) correction of situations at risk, 4) integration of OHS into purchasing, 5) arrangement of safety monitoring devices (planning and registries), 6) presence of proper means of response to emergency situations (emergency supplies and personnel), 7) documentation of occupational lesions and, 8) company physician intervention protocol.
Implementing the OHSMS implies a formal commitment by the company to comply with the legal obligations and thus favors continued improvement of work conditions [116] Compliance with the LSST by itself improves the company brand image [113]. Four factors that determine the success of the system are 1) upper management is on board, 2) commitment to the principle of continued improvement, 3) worker participation, and 4) internal communication [121]. Other factors, perhaps more difficult to verify, are the suitability of the system for the company, the effectiveness of audits, and proper definition of the responsibilities of the stakeholders [114].
The elements of an OHS management system that ultimately have the most influence on OHS performance are summarized in Figure 6.
Figure 6. Summary of the most influential elements of management systems on OHS performance
3.2.4 Implementation of occupational health and safety
The employer, the workers, and the shareholders are the principal stakeholders in the implementation of OHS. This process consists of establishing measures that enable a business to identify, correct and control OHS risks adequately [122]. It must aim to promote worker participation.
Implementation by managers. OHS historically has not been a major preoccupation in SMEs or a priority of their managers [123]. In fact, managers of many of these businesses used to attach little importance to OHS management [36]. This attitude is even more apparent in the most dangerous industries [94]. The OHS performance of SMEs rests on the ability of managers to involve their prevention teams [34]. Studies focused on SMEs have revealed close relationships between managerial traits (conscientiousness, perceptiveness, leadership) and company performance [124]. The deficiencies of managers appear in many cases to be major obstacles to the improvement of OHS [91].
Managers in SMEs often do not feel responsible for the well-being of workers. When an occupational ailment or injury occurs, they view the worker and not OHS management as the cause [8]. The occurrence is attributed to worker inattentiveness or carelessness in the presence of a known hazard [36]. These managers say that it is a complicated matter to see to prevention when the workers themselves are not convinced of the need for it [125].
Managers of SMEs generally do not possess knowledge or know-how in the management of prevention [89] or efficient evaluation and monitoring of OHS risks [88, 45]. They tend to work long hours, 50 to 70 per week [126], which leaves them little time to improve their knowledge of OHS, certainly not by reading scientific journals, even when they are capable of understanding the language of scientific publication. According to a relatively recent survey, 32.7% of directors of SMEs have completed high school or less, 32% have a college diploma, 22.5% have a bachelor’s degree and 12.6% have a graduate degree [7].
Implementation by workers. Prevention and its management are always more effective when the workers get involved actively [127]. This will occur if the workers perceive their contribution as being recognized and utilized by their managers [128]. In SMEs, it is always difficult to get workers involved in prevention, even when mechanisms such as health and safety committees are mandatory. Not all workers are able to exercise their right refuse to work in the presence of hazards, in some cases because they are younger or less educated, or rotation is too frequent to allow them to become familiar with the hazards associated with tasks or even be aware of risks that may be serious [94].
The case of migrant workers in Quebec SMEs shows that risks are often ignored, and diseases or injuries go undeclared [129]. Most of these workers are unaware of their rights and obligations regarding OHS, usually as a direct result of the language barrier. Even when the working conditions carry obvious risks of harm, it is assumed that complaining will result in dismissal [129]. Immigrants also do not assert certain OHS rights [130], and economic pressures push them towards acceptance of more hazardous work [131].
OHS training. Training is one of the most frequently chosen elements of prevention programs in businesses [132-134] and has a positive and concrete impact on OHS performance, largely by improving worker attitudes and behavior, raising awareness of hazards and health risks [135], developing knowledge in prevention and thereby increasing willingness and the effectiveness of employees involved in the program [136-139] and reducing the overall prevalence of occupational diseases [140].
OHS training takes place upon hiring and in various forms throughout the year [135]. Training programs vary considerably in the level of worker participation [141], which may be minimal (simple sharing of information), moderate (utilizing participant experience) or extensive (simulations with emphasis on the practical application of concepts), the latter type being the most effective. In SMEs, training in OHS should be in-house and more strongly oriented towards practice, since intensive learning of theory in classrooms has been found not very effective for this setting [35].
Instructor characteristics also influence the success of OHS training [140, 142]. The instructors must be apt teachers and regarded as knowledgeable and competent with real experience on the jobs of the workers [141]. The training must be well organized and easy to apply immediately in the workplace [143], and the equiSMEnt, devices and materials required to do so must be readily available [144]. Follow-up with the workers trained is also important.
OHS training in SMEs has been insufficient [145] and mostly informal and poorly organized [146]. Based on how much the owners of these businesses participate in the training, it must be concluded that they have been unconvinced of its value.
Auditing, inspections and monitoring. Monitoring and investigation are important elements of the avoidance of occupational diseases [15, 40, 110, 122, 135]. Risks and dysfunctions in the workplace are relatively easy to identify by maintaining a proper system of inspections [147], without which effective OHS management is not possible.
In SMEs, required OHS measures comprise essentially workplace monitoring and inspection of risks as well as preventive maintenance [110]. This should include systematic checking of collective protection equiSMEnt, particularly ventilation systems, common areas and hygienic conditions that workers face [15]. However, inspections of any type have been rare in SMEs [148].
Figure 7. Summary of the elements of practice identified as influencing OHS performance
Medical examinations. The following types of medical examinations may be conducted routinely: before hiring, regular check-up, unannounced, extended, upon return to work, checking for specific situations [149].
Pre-hiring examination may be required in the process of determining if a worker is fit to perform the task to which he/she will be assigned and is able to comply with the associated specific preventive measures [149] and/or if he/she has any ailment or medical/physical condition that could be worsened by performing that task [150]. These examinations also provide the opportunity to update preventive measures applied at the workstation and disseminate information on the hazardous situations that can arise while performing specific tasks [151]. Unannounced examinations take place on demand by a worker, for example, if a health concern makes him/her feel unfit to engage in certain activities [149]. Extended examinations are applicable to workers that are exposed regularly to certain risks (chemical, biological, etc.). Examination is also indicated for a worker returning to his/her job after four or more consecutive weeks of absence to recover from an occupational ailment and for such workers being assigned to a new workstation. Job categories requiring specific medical testing include night shifts, work at noise levels exceeding 85 dB, and tasks involving exposure to any carcinogen, mutagen, or neurotoxic substance [152].
The elements of practice identified as influencing OHS performance are summarized in Figure 7.
3.2.5 Workplace and work organization
The workplace and the work that takes place therein are generally organized according to what management believes will maximize productivity [153]. Organization includes work pace, production systems, and management of subcontracting [154] as well as shift scheduling and salary structure [155]. Effects of organizational deficiencies on worker health are well known to exist [154, 156]. Improvement of workplace and work organization thus represents an important lever for dealing with the problem of occupational diseases [154].
Managers of SMEs tend to attribute OHS-related difficulties to factors external to the company, such as taxes, inflation, and other economic parameters [45] and are disinclined to consider internal factors such as organization, work conditions or scheduling, salary, work social environment, over which they have at least some control [157].
Work scheduling. The work week of a wage earner is generally 40 hours, although this may vary from one business to another and with the type and seasonality of the activities. Some businesses function for 35 or 39 hours per week not counting overtime [158]. Work shifts in SMEs are often longer, with work weeks exceeding 40 hours [159].
Work scheduling can have a direct effect on worker health [160, 161]. Studies have shown that workers who spend 48 hours or more per week on the job can suffer from psychological, cardiovascular, or digestive problems [162]. Many workers opt for night shifts to increase their pay [163]. Working nights only can lead to cardiovascular problems and cancers, especially breast and colorectal, and constant nighttime exposure to light appears to weaken the immune system [164]. However, the health of workers on atypical schedules has not been well documented [165] and OHS science has yet to address this category of workers adequately.
Subcontracting and temporary work. Subcontracting in SMEs often exposes workers to OHS risks. Many managers have used the threat of replacing permanent staff with subcontractors to improve business competitiveness without giving due consideration to OHS [166], a practice that has received much attention from researchers because of its proven impact on OHS [167]. Companies can use this ploy to duck their OHS obligations. The temporary workers (employees of the subcontractor) are often subjected to bad working conditions involving constrained postures, repetitive movements, handling of heavy loads, faster work pace, and so on [168]. In addition, these workers tend to be poorly trained, less familiar with the work site and processes, and are often given the most dangerous tasks [169].
Labor union organization and social climate. Most employees of SMEs are not unionized. In Quebec, 79.4% of small businesses have no unionized employees [170]. SMEs with no labor union have no system of monitoring by labor and management to oversee prevention practices [171]. Occupational ailment risk factors, particularly disregard of exposure limits (chemical, radioactive, thermic), have been on the rise in non-unionized SMEs in Quebec [172]. Lunch and coffee break times are often not applied consistently, and workers are given repetitive tasks that require much physical effort. Injuries and diseases are underreported.
A lack of support from managers increases mental health problems among workers, especially depression and anxiety [173]. The support of the supervisor improves job satisfaction [174]. Chronic pathologies of joints and bones can result from psychosocial pressures in the workplace [175]. Research has shown that poor social support can ruin health [173]. Workers under such conditions feel more stress and more symptoms of burnout.
The social climate in SMEs depends largely on the company directors [123]. Proximity of workers and managers can have a positive influence [176]. Relations are generally informal in SMEs [177, 178], which can be beneficial since managers have to balance authoritarian discipline and closer social relations with workers. However, informality also makes unionizing and hence OHS initiatives less likely [179].
Where the social climate is strained, there will be no chance for OHS culture to develop. Advice from a colleague on work methods or reminders of the proper use of personal protective devices will not be welcome [94].
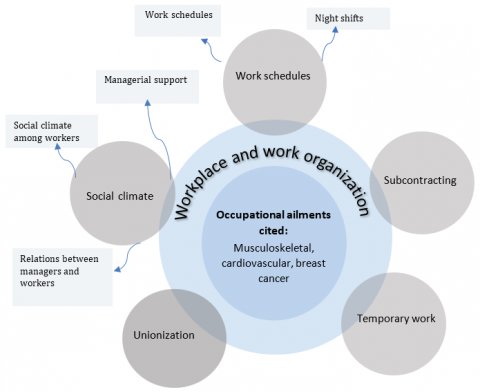
The elements of workplace and work organization that influence OHS performance are summarized in Figure 8.
3.2.6 Management of occupational risks
Occupational risk encompasses hazards that can affect the health (mental or physical) or the safety of workers [180]. The CNESST (2016) groups risks encountered in the workplace into six categories: 1) chemical, 2) biological, 3) physical, 4) ergonomic, 5) safety, and 6) psychosocial. In the present study, we focus on physical health in relation to occupational diseases, which is associated mainly with the first four categories of risk named by the CCHST (2018).
Whereas workers are more exposed to occupational risks in SMEs than in large corporations [39, 42, 88], the ability of these smaller companies to manage the risks is limited [43, 88] and the means used to do so are poorly adapted to the risks that the workers actually face [181, 182]. SMEs do not have specific methods at their disposal or much grasp of the principles of risk appreciation [183] or sufficient resources to implement measures addressing occupational risks [87, 88]. How health and safety risks are perceived has a strong influence on how they are managed [183]. Perception influence communication, acceptance, evaluation and control of risks [184] and is often false [16, 184]. Managers of SMEs often underestimate risks and invest little in their management [45], instead associating them with worker carelessness, non-use of personal protective devices, voluntary engaging in unsafe behavior, and so on [4]. Workers usually are not aware of the risks to which they are exposed and tend to ignore them [45].
Figure 8. Summary of the elements of workplace and work organization that influence OHS performance
Management of chemical risks. According to a study of the years 2005 to 2007, the use of chemicals in the workplace in Quebec caused 1,500 lesions or diseases, of which 350 were associated with occupational diseases. In Quebec, the six main categories of occupational disease caused by chemical substances are: 1) asbestosis, 2) mesothelioma, 3) eczemas, 5) cancer, 5) silicosis, and 6) occupational asthma.
The management of chemical risks can be resumed in four steps [110, 185]: 1) identification of the dangerous materials used in the workplace and the risks associated, 2) evaluation of the seriousness, 3) devising and implementing corrective actions, and 4) monitoring the actions for consistency of applications and effectiveness.
Canada has its workplace hazardous material information system (WHMIS), of which the current version (2015) is largely in step with the General harmonized system (GHS). Suppliers, employers and workers all have a stake in the Workplace Hazardous Materials Information System (WHMIS) [110]. The supplier provides up-to-date information on the hazards labels and the safety data sheets. The employer must ensure that all dangerous materials, chemicals or substances used on his premises bear the proper label and that the safety data sheets are nearby. If the company itself manufactures the product, the employer is solely responsible for preparing the product label and safety sheet. It is the employer’s duty to establish the required training and information program for the storage, transport and use of the product. Workers must take the training, attend all information sessions, and ensure their protection as well as that of their colleagues. Workers have the responsibility of taking part in the identification and elimination of chemical risks.
Exposure to chemical risks is higher in SMEs than in large corporations [42, 123]. Management of dangerous materials in SMEs has been mediocre overall [186]. Exposure to carcinogens is higher on average in SMEs [187]. Managers either lack the applicable competency or do not wish to use them to manage chemical risks [188], often not understanding the information provided by suppliers or not applying it adequately [188]. Workers often do not know that the products to which they are exposed are dangerous [186]. The long-term consequences of exposure to dangerous products are less often explained in SMEs [186, 189].
Evaluating chemical risks consists of analyzing the conditions of exposure of workers to hazards primarily by noting the workstations at which the substances or materials are used, and then examining in detail the processes (quantity, temperature, pressure, etc.) in which they are involved [151].
The most effective corrective measure would be to eliminate the dangerous substance or material, by replacing it with a less dangerous substitute [151]. However, such substitutions are fraught with complexities, such as technical feasibility, cost, supply and quality stability, and human resource availability, which may be daunting [190]. In general, SMEs do not have the financial means or expertise necessary to replace materials or reagents with safer substitutes [187].
Collective protection against chemical risks can be achieved through the application of technical and organizational measures. Upgrading ventilation systems and containment, introducing safe work methods, limiting access to hazardous zones, mechanizing and automating processes, and describing in detail all maintenance and servicing procedures, all contribute to reducing exposure time and intensity.
Training, information, and raising awareness also are in the category of collective measures. Certain aspects of chemical risks must be spelled out to workers: which products are dangerous, where exposure occurs, and so on. They must be familiarized with the safety considerations applicable to their workstation and the associated collective and personal protective devices and emergency procedures. Chemical risk management is also strengthened by simple hygienic measures: hand-washing, wearing clean work clothes and keeping work area tidy. Training and information are effective if they are adapted to the work setting (conditions, station, dangerous substances present, etc.). Training must be practical and easily understood. During training, workers must participate and express the reality of their constraints.
Personal protective devices are recommended wherever corrective measures at the source of exposure do not ensure adequate protection of workers [191]. However, it must be kept in mind that these devices constitute the least effective risk control measures [192, 193]. They nevertheless contribute to the prevention of certain lesions and occupational diseases [40, 192-194]. Good examples of this are safety glasses [195], breathing masks, protective clothing [196] as well as gloves and safety footwear [110, 196]. Personal devices are effective when used in the situation for which they were designed [191, 197, 169], do not cause discomfort (heat, skin irritation, etc.) or clumsiness [191, 196, 197] are properly fitted to the user [197] and in new or close to new condition [122].
Personal devices are the most common risk management element used in SMEs [194]. And yet some researchers have found that even these means are not always available in this setting [198]. When they are, managers are not always able to persuade the workers to wear them [199]. In addition, restrained budgets preclude obtaining the most adequate devices [186]. In summary, SMEs have fewer human resources and less technical competency, time and tools to manage chemical risks effectively [200].
Management of biological risks. Biological risks are associated with living organisms (bacteria, yeasts, fungi, parasites, etc.) and replicating entities (viruses, prions) that can affect the health of workers [110]. During the years 2005 to 2007, biological agents were the cause of 1,360 lesions per year and 80 cases of occupational disease. Exposure to biological agents can cause skin lesions, pneumonia, cancers, and other debilitating conditions [151].
The six principal means of managing biological risks [110, 201, 202] are: 1) use of safety equiSMEnt, 2) use of protective devices (individual and collective), 3) adoption of safe work methods, 4) rigorous application of hygienic practices (handwashing, cleaning and sterilization of tools, etc.), 5) raising awareness, and 6) vaccination of exposed workers.
Management of physical risks. Physical risks to workers are associated with noise, vibrations, radiation, electricity, and temperature extremes [110]. Hearing loss is a major OHS preoccupation in Quebec [203, 204]. Exposure to noise is also a cardiovascular health risk factor [205]. In Quebec, about 7% of employees of small businesses and 13.4% in medium-sized businesses are exposed continually to noise [170]. By provincial regulation, no worker is to be exposed to continual noise exceeding 90 dB during an eight-hour work shift (A). By federal regulation (A), the limit is 87 dB [197].
Exposure to noise comprises three elements: sources (tools and machines), the medium of transmission, and the receptor, namely eardrums [206-208]. The manager must develop a noise exposure reduction plan (April, 2007) focused on all three elements.
Eliminating noise at the source (mainly machinery) is the first line of intervention [203]. Regular servicing of all mechanical devices (changing worn or corroded parts, lubrification, etc.) lowers noise by 1 to 10 dB (A) and if carried out systematically constitutes preventive maintenance [208]. Replacing (upgrading) noisy equiSMEnt and processes or procedures and optimizing operating speeds and pressures are other effective interventions.
The transmission of noise can be attenuated by sound-absorbing screens, cabinets, enclosures and so on [151, 207]. These elements are incorporated into the work areas ideally during the design of the facility [209]. Sources of noise should be placed as far as possible from workers and in spaces other than work areas. Ceilings and floors should be fitted with noise-absorbing materials.
Measuring noise levels is essential for identifying the workers most exposed [207] and making sure that these employees are provided with adequate auditory protection [206, 208]. Organizing work schedules to reduce the time of exposure and the number of workers exposed to the worst noises is also helpful [208].
Exposure to noise is frequently very high in SMEs [210], and controlling noise is not a priority [211]. This is partly because managers of SMEs do not know how to determine which measures would be the most effective economically. They also tend to prefer auditory protection over administrative or technical measures [186, 212], viewing the latter as too expensive for their businesses [88]. However, protectors are seldom adequate by themselves [212], and it has proven difficult for SMEs to implement individual measures or even determine which workers would benefit most from these [213]. This task is complicated by a lack of know-how in noise exposure evaluation and further by intermittent exposure [213].
Exposure to radiation can cause several occupational diseases, such as cancer and cataracts [214]. According to the Canadian nuclear safety committee (2016), workers in Quebec are exposed to two categories of radiation: of artificial origin (encountered in research and develoSMEnt laboratories and in some manufacturing industries, the nuclear industry, etc.), and of natural origin (in mining, construction, etc.).
The Ontario Labor Ministry has proposed five elements of management of exposure to radiation: 1) preventing or limiting the dispersion of ultraviolet rays using opaque materials (wood, cardboard, etc.), 2) limiting exposure time and distancing workers from sources of radiation, 3) using signs that indicate where radiation may be propagated, 4) providing workers with adequate protective devices (glasses, clothing, sunscreen, etc.) and 5) protecting employees who work outdoors (limiting exposure time, providing protective devices).
Exposure of upper limbs or the entire body to vibrations affects respectively 8.9% and 5.6% of Quebec workers aged 15 to 29. Among those aged 30 or more, the numbers are 6.6% and 5.1% [215]. One of the most common consequences is Raynaud’s disease [216]. Neurological disorders and musculoskeletal pain are also reported [217]. Solutions to the problem of worker exposure to vibrations have been proposed in several studies [151, 216-219]. Upgrading vibrating equiSMEnt and the floors or surfaces on which workers are stationed or circulate, though effective at reducing the transmission of vibrations, involve proper monitoring and maintenance, in addition to adjusting vehicle speeds to the new surfaces. Suspension chairs or cabinets help, but also need maintenance to remain effective. Workstations can be rearranged to reduce the time of exposure, in conjunction with proper training and raising of awareness among workers.
Again, exposure to vibrations is greater in SMEs than in the employ of large corporations [170, 220]. This is the case notably for upper limbs [42].
During the years 2012 to 2016, 95 Quebec workers suffered lesions caused by cold temperatures [221]. During the same period, 18 workers suffered lesions caused by heat [110]. Coldness makes work onerous, increases fatigue, and reduces sensitivity. Workers in cold conditions may also have trouble moving, communicating, and avoiding hazards [222]. The danger of frostbite and hypothermia obviously looms [223]. The effects of heat may evolve through four states: 1) rashes, pain, and fever, 2) muscle cramps, dehydration, and wavering consciousness, 3) exhaustion, sweating, and decreased pulse, and 4) heatstroke, increased pulse, and unconsciousness [52].
The solutions to problems of cold and hot working environments are based first on work organization [110, 222, 224, 225]. Alternating work and rest, teamwork, supervising workers, distributing tasks according to ambient conditions. Workstation design and furnishings can often be improved, temperature can be managed with air conditioning or ventilation [225], and tasks can be automated [224]. When avoidance of exposure to heat is not possible, workers must have access to good drinking water ad libitum [224]. All special clothing and protective accessory options must also be considered [110, 222, 224, 225].
Electrical risks arise primarily in three forms: shock from ungrounded circuits, electrocution, and burning [151]. In Quebec, one worker per week suffers a shock or electrocution [110]. Electrical current passing through the body can cause loss of balance, external and internal injury, and damage to the lungs and heart, and obviously can be fatal [151]. Electrical arcs can cause losses of hearing eyesight, open wounds, contusions, and bone fractures [226].
The first preventive measure is to intervene at the source. Power must be easy to shut off, and proper electrical insulation must be installed between the worker and the electrical source [151, 226]. Workers exposed to electrical hazards must wear dielectric gloves, insulated footwear, anti-arc visors and so on. Lockout/tagout protocols (with padlocks on power switches) play a major role in protection against electrical hazards (110). Finally, if servicing or maintenance operations require power ON, the technician must hold a permit to work on powered machinery, in compliance with CSA standard Z462, a 4.3.2.2, which permit includes 11 main elements, including management of electrical risks.
Management of ergonomic risks. Ergonomic risks are associated with repetitive movements, intense physical efforts, and unnatural postures (110). Workstation design, production processes, and work organization and methods have less direct effects but are nevertheless important factors in this category of occupational risk [227, 228]. The main diseases associated with poor ergonomics are musculoskeletal pains and trauma [229], which account for a large proportion of work disability in Quebec [230], affecting about 20% of workers in small businesses and 24.8% in medium-sized businesses [170]. Means of managing musculoskeletal risks focus on five main elements: surroundings, equiSMEnt and tools, the tasks, the worker, organization, and resource management [231].
Work area set up (arrangement, space, etc.) must be designed to prevent musculoskeletal wear and tear [232]. Workstations must be adaptable to the individual worker (adjustable chairs and table height and width). Work areas must have adequate lighting, whether natural, artificial or a combination of the two [169]. Poor lighting can cause fatigue and visual discomfort [233] and make the worker adopt awkward and harmful postures [234] or lean too close to machinery, materials, conveyors and so on [235].
EquiSMEnt and tools must be adjustable to the worker [231]. Tools should be assisted (with supports) and lightweight. Certain characteristics such as handle diameter and shape and surface texture can also be optimized to reduce musculoskeletal risk factors [197].
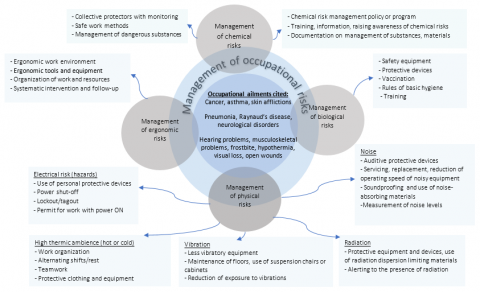
Figure 9. Summary of the elements of occupational risk management influencing OHS performance
The worker must not be solicited beyond his/her physical capacities [236]. The risk of developing a musculoskeletal disease must be anticipated and evaluated constantly [236, 237]. Several methods are available for this, for example, proposed in the NIOSH guide to lifting. These also will suggest corrective measures (modification of workstations, work pace, etc.) when unacceptable work conditions are found [132, 231].
Employee training plays a fundamental role in the prevention of musculoskeletal diseases [234, 238]. In some cases, the services of an external consultant may be necessary to obtain the desired results [228]. Training in the proper handling of heavy loads used to be one of the most frequent requests made to experts in ergonomics [238]. Training must also teach the basic principles of ergonomics, musculoskeletal risk factors, and approaches to modifying the ergonomics of workstations and tasks [228]. The reduction of musculoskeletal risk factors is a complementary element of the training [239]. Employees must participate in the identification and analysis of musculoskeletal risk factors and the implementation of preventive measures [240]. Their awareness of this type of risk must also be raised, to ensure that they put the measures into practice [231].
One effective approach to preventing musculoskeletal diseases is job rotation [234, 241, 242]. Work organization also encompasses respecting lunch hours and rest periods, as well as better scheduling of tasks [231]. Resting during shifts is discouraged more often in SMEs [170]. Managers must be prepared to invest financially in prevention, to ensure that sufficient human resources are available to make preventive measures feasible.
Research has shown that employees handle larger physical loads in SMEs than they do in large corporations [170]. Employees more frequently handle large loads in the SME setting and perform repetitive tasks requiring tools or equiSMEnt and physical exertion often in a standing position. Methods of ergonomic analysis of tasks (posture, repetitiveness, etc.) have been found too specialized and not adapted to SME reality [243]. Furthermore, the cost of some of the ergonomic interventions proposed is not affordable in these businesses [90].
The elements of occupational risk management that influence OHS performance is summarized below in Figure 9. The details of all elements of managing occupational ailment prevention mentioned above are listed in a spreadsheet file (Excel worksheets, in French only) available with the present article.
3.3 Limitations of this study; prospects for future work in this subject area
Several of the managerial elements of prevention identified in this review of the literature do not apply specifically to the SME context or even to risks of developing occupational diseases. These elements concern, at least in part, risk management in large corporations.
The results of this literature search will provide a starting point for a more in-depth research project focused on OHS in small and medium-sized businesses. For example, develoSMEnt of a decision aid tool more accessible to and better designed for SMEs could be guided by the information summarized in this article. We believe that research along these lines will help to achieve the goal of improving the protection of workers exposed to myriad hazards in the increasingly complex and dynamic work environments of modern economies.
Occupational injuries, lesions, diseases, illnesses, and diseases engender human and social costs, hidden and visible. Absenteeism for health and medical reasons increase salary costs, insurance costs, administrative burden, and decreases national economic productivity and competitiveness. Recent statistics show that the number of workplace accidents has been decreasing, unlike occupational diseases, which are increasing steadily. The number of deaths caused each year by occupational diseases is now greater than the number caused by workplace accidents.
The goal of this study was to catalog the interventions most widely practiced as management of the risk of developing occupational diseases in small and medium-sized manufacturing enterprises in Quebec. This review of the literature allowed us to identify about a hundred elements of occupational ailment and disease prevention. These are examined more closely in the second part of this research, which focuses on the details of their actual application in the SME setting [1]. The project overall allowed us to identify the strengths and deficiencies of OHS risk management in these businesses.
[1] Randrianarivelo, R., Badri, A., Gauthier, F., Boudreau-Trudel, B. (2022). Prevention of occupational diseases in small and medium-sized manufacturing enterprises in Quebec (Canada) - Study of prevention management practices. International Journal of Safety and Security Engineering, 12(3): 279-289.
[2] Organisation de coopération et de développement économiques. (2000). Les petites et moyennes entreprises: Force locale, action mondiale. L’observateur. OCDE. Consulted June 8, 2021: http://www.oecd.org/fr/industrie/SME/1918323.pdf.
[3] Mahé De Boislandelle, H. (1998). GRH en PME: universalité et contingences: essai de théorisation. Revue Internationale PME Économie et Gestion de la Petite et Moyenne Entreprise, 11(2-3): 11-30. https://doi.org/10.7202/1009041ar
[4] Martin, C. (2008). Contribution à la définition d'actions pour la pérennisation de la prévention des risques professionnels dans les PME-PMI. Doctoral Dissertation, École Nationale Supérieure des Mines de Paris. https://pastel.archives-ouvertes.fr/tel-00352172/document
[5] Institut de la Statistique du Québec. (2015). Petites et moyennes entreprises (SME). Gouvernement du Québec. Consulted May 2, 2021: http://www.stat.gouv.qc.ca/statistiques/science-technologie-innovation/financement_SME/cdmi.html
[6] Vallée, P. (2013). Dans SME, le P est beaucoup plus grand que le M ! Le Devoir. Consulted July 16, 2021: http://www.ledevoir.com/economie/actualites-economiques/390731/dans-SME-le-p-est-beaucoup-plus-grand-que-le-m
[7] Lord, S. (2016). Quelle est la part des SME dans l’économie ? La presse. Consulted June 22, 2021: http://affaires.lapresse.ca/SME/201610/05/01-5027546-quelle-est-la-part-des-SME-dans-leconomie-.php
[8] Vickers, I., James, P., Smallbone, D., Baldock, R. (2005). Understanding small firm responses to regulation: the case of workplace health and safety. Policy Studies, 26(2): 149-169. https://doi.org/10.1080/01442870500127626
[9] Leblanc, M. (2015). La relève en PME: un enjeu vital pour l’économie du Québec. Gestion, 40(2): 24-26. https://doi.org/10.3917/riges.402.0024
[10] Fontaine, J. (2013). Les lésions professionnelles coûtent 4,6 G$ par an au Québec. Les Affaires. Consulted July 14, 2021: http://www.lesaffaires.com/strategie-d-entreprise/management/les-lesions-professionnelles-coutent-46-g-par-an-au-quebec/554401
[11] Duguay, P., Boucher, A., Busque, M.A. (2017). Statistiques sur les maladies professionnelles au Québec. Colloque IRSST–Maladie professionnelles: portrait, défis et perspectives. Consulted July 14, 2021: http://www.irsst.qc.ca/publications-etoutils/video/i/100251/n/statistiques-maladies-professionnelles-quebec/redirected/1
[12] Labrèche, F., Duguay, P., Ancand, R., Boucher, A. (2013). Estimation du nombre de cancers d’origine professionnelle au Québec. (R-789). Montréal, Canada: IRSST. Consulted May 2, 2021: http://www.irsst.qc.ca/media/documents/PubIRSST/R-789.pdf
[13] Commission des normes, de l’équité, de la santé et de la sécurité du travail et Institut de recherche Robert-Sauvé en santé et en Sécurité du travail. (2016). Premiers indicateurs annuels de lésions professionnelles. Prévention au Travail, 29(94): 17-20.
[14] Duguay, P., Boucher, A., Busque, M.A. (2014) Statistiques sur les maladies professionnelles au Québec. Colloque IRSST–Maladie professionnelles: portrait, défis et perspectives. Consulted July 14, 2021: http://www.irsst.qc.ca/publications-etoutils/video/i/100251/n/statistiques-maladies-professionnelles-quebec/redirected/1
[15] Gopang, M.A., Nebhwani, M., Khatri, A., Marri, H.B. (2017). An assessment of occupational health and safety measures and performance of SMEs: An empirical investigation. Safety Science, 93: 127-133. https://doi.org/10.1016/j.ssci.2016.11.024
[16] Cagno, E., Micheli, G.J., Perotti, S. (2011). Identification of OHS-related factors and interactions among those and OHS performance in SMEs. Safety Science, 49(2): 216-225. https://doi.org/10.1016/j.ssci.2010.08.002
[17] Tremblay, A., Badri, A. (2018). Assessment of occupational health and safety performance evaluation tools: State of the art and challenges for small and medium-sized enterprises. Safety Science, 101: 260-267. https://doi.org/10.1016/j.ssci.2017.09.016
[18] Hellemans, C., Piette, A., Himpens, A. (2010). Un outil complet pour l’analyse des facultés de travail des travailleurs vieillissants. Travail et Santé, 26(3): 1-8.
[19] Mendeloff, J., Nelson, C., Ko, K., Haviland, A. (2006) Small businesses and workplace fatality risk: An exploratory analysis (Rand TR 371) California, Rand Corporation. Consulted June 12, 2021: https://www.rand.org/content/dam/rand/pubs/technical_reports/2006/RAND_TR371.pdf
[20] Liu, Y.J., Chen, J.L., Cheng, S.Y., Hsu, M.T., Wang, C.H. (2014). Evaluation of safety performance in process industries. Process Safety Progress, 33(2): 166-171. https://doi.org/10.1002/prs.11644
[21] Dı́az, R.I., Cabrera, D.D. (1997). Safety climate and attitude as evaluation measures of organizational safety. Accident Analysis & Prevention, 29(5): 643-650. https://doi.org/10.1016/S0001-4575(97)00015-8
[22] Wu, T.C., Chen, C.H., Li, C.C. (2008). A correlation among safety leadership, safety climate and safety performance. Journal of Loss Prevention in the Process Industries, 21(3): 307-318. https://doi.org/10.1016/j.jlp.2007.11.001
[23] Roy, M., Desmarais, L., Cadieux, J. (2005). Améliorer la performance en SST: les résultats vs les prédicteurs. Perspectives interdisciplinaires sur le travail et la santé, (7-2). http://dx.doi.org/10.4000/pistes.3214
[24] Arezes, P.M., Sérgio Miguel, A. (2003). The role of safety culture in safety performance measurement. Measuring Business Excellence, 7(4): 20-28. https://doi.org/10.1108/13683040310509287
[25] Fortin, C. (2015). Le contrôle des risques et la mesure de la performance en santé au travail. 37e Congrès de l’AQHSST. Saint-Sauveur: AQHSST.
[26] Dionne-Proulx, J., Carrière, J.B., Beauchamp, Y. (2003). ISO 9000 et après: impact sur la performance en SST dans l’entreprise manufacturière: Rapport. (R 327). Montréal, Canada : IRSST. Consulted June 22, 2021: http://www.irsst.qc.ca/media/documents/pubirsst/R-327.pdf
[27] Cambon, J., Guarnieri, F., Groeneweg, J. (2006). Towards a new tool for measuring safety management systems performance. In Proceedings of the Second Resilience Engineering Symposium. Mines Paris, Less Presses, Antibes–Juan-les-Pins, France, pp. 53-62.
[28] Sinelnikov, S., Inouye, J., Kerper, S. (2015). Using leading indicators to measure occupational health and safety performance. Safety Science, 72: 240-248. https://doi.org/10.1016/j.ssci.2014.09.010
[29] Podgórski, D. (2015). Measuring operational performance of OSH management system–A demonstration of AHP-based selection of leading key performance indicators. Safety Science, 73: 146-166. https://doi.org/10.1016/j.ssci.2014.11.018
[30] Lingard, H., Wakefield, R., Cashin, P. (2011). The develoSMEnt and testing of a hierarchical measure of project OHS performance. Engineering, Construction and Architectural Management, 18(1): 30-49. https://doi.org/10.1108/09699981111098676
[31] Erikson, S.G. (2009). Performance indicators. Safety Science, 47(4): 468.
[32] Hopkins, A. (2009). Thinking about process safety indicators. Safety Science, 47(4): 460-465.
[33] Shea, T., De Cieri, H., Donohue, R., Cooper, B., Sheehan, C. (2016). Leading indicators of occupational health and safety: An employee and workplace level validation study. Safety Science, 85: 293-304. https://doi.org/10.1016/j.ssci.2016.01.015
[34] Gravel, S., Vergara, D., Lippel, K., Dubé, J., Ducharme-Varin, J.F., Legendre, G. (2016). Santé et sécurité des travailleurs qui cumulent des précarités: la lutte aux inégalités de santé attribuables au travail. Health and safety of workers with accumulated precariousness: tackling work-related health inequalities). Montréal: Centre de recherche Léa-Roback sur les inégalités sociales de santé de Montréal, 60.
[35] Farvaque, N., Voss, E., Lefebvre, M., Schütze, K. (2009). Guide for training in SMEs. DG Employment. Social Affairs and Equal Opportunities, France, pp. 18-53.
[36] Martin, C., Guarnieri, F. (2008). Position du problème. Pratiques de prévention des risques professionnels dans les SME-PMI. in Technique & Documentation-Lavoisier. Paris: Lavoisier. Consulted June 18, 2021: https://www.researchgate.net/publication/278767241_Pratiques_de_prevention_des_risques_professionnels_dans_les_SME-PMI
[37] Frazier, C.B., Ludwig, T.D., Whitaker, B., Roberts, D.S. (2013). A hierarchical factor analysis of a safety culture survey. Journal of Safety Research, 45: 15-28. https://doi.org/10.1016/j.jsr.2012.10.015
[38] Lescure, E., Nadeau, S., Morency, F. (2015). SME et SST: Quand la résilience est un modèle d’affaires. 50e Congrès international de la société d’Ergonomie de Langue Française. Paris: Société d’Ergonomie de Langue Française. Consulted May 2, 2021: http://espace2.etsmtl.ca/id/eprint/11459/1/Morency%20F.%202015%2011459%20SME%20et%20SST%20Quand%20la%20r%C3%A9silience%20est%20un%20mod%C3%A8le%20d%27affaires.pdf
[39] Legg, S.J., Olsen, K.B., Laird, I.S., Hasle, P. (2015). Managing safety in small and medium enterprises. Safety Science, 71: 189-196. https://doi.org/10.1016/j.ssci.2014.11.007
[40] Champoux, D., Brun, J.P. (1999). Prise en charge de la sécurité dans les petites entreprises des secteurs de l’habillement et de la fabrication de produits en métal. Institut de recherche en santé et en sécurité du travail du Québec, 1-26
[41] Cunningham, T.R., Sinclair, R. (2015). Application of a model for delivering occupational safety and health to smaller businesses: Case studies from the US. Safety Science, 71: 213-225. https://doi.org/10.1016/j.ssci.2014.06.011
[42] Sørensen, O.H., Hasle, P., Bach, E. (2007). Working in small enterprises–is there a special risk? Safety Science, 45(10): 1044-1059. https://doi.org/10.1016/j.ssci.2006.09.005
[43] Micheli, G.J., Cagno, E. (2010). Dealing with SMEs as a whole in OHS issues: Warnings from empirical evidence. Safety Science, 48(6): 729-733. https://doi.org/10.1016/j.ssci.2010.02.010
[44] Targoutzidis, A., Koukoulaki, T., Schmitz-Felten, E., Kuhl, K., Hengel, K.M.O., Rijken, E., Klüser, R. (2014). The business case for safety and health at work: Cost-benefit analyses of interventions in small and medium–sized enterprises–study. Office of the European Union, Luxembourg. Consulted July 18, 2021: https://publications. europa. eu/en/publication-detail/— /publication/8e9e23ea-2270–4d51 –8553–94152e503afd
[45] Champoux, D., Brun, J.P. (2003). Occupational health and safety management in small size enterprises: an overview of the situation and avenues for intervention and research. Safety Science, 41(4): 301-318. https://doi.org/10.1016/S0925-7535(02)00043-7
[46] Sönderstrup-Andersen, H., Flöcke, T., Mikkelsen, K., Roepstorff, C. (2010). Measuring enterprise proactiveness in managing occupational safety. Safety Science Monit, 14(1): 1-8.
[47] Wilson, J.M., Koehn, E.E. (2000). Safety management: problems encountered and recommended solutions. Journal of Construction Engineering and Management, 126(1): 77-79. https://doi.org/10.1061/(ASCE)0733-9364(2000)126:1(77)
[48] Galia, F. (2003). Compétences et gestion des ressources humaines de l'industrie française dans une perspective d'innovation. l’université Paris-Dauphine, 1-17
[49] Freitas, A.C., Silva, S.A. (2017). Exploring OHS trainers’ role in the transfer of training. Safety Science, 91: 310-319. https://doi.org/10.1016/j.ssci.2016.08.007
[50] Morse, T., Dillon, C., Weber, J., Warren, N., Bruneau, H., Fu, R. (2004). Prevalence and reporting of occupational illness by company size: population trends and regulatory implications. American Journal of Industrial Medicine, 45(4): 361-370. https://doi.org/10.1002/ajim.10354
[51] Ukai, H., Okamoto, S., Takada, S., Yamada, C., Ikeda, M. (2004). Lower vapor concentrations in solvent workplaces in larger-scale enterprises than in smaller-scale enterprises, and exceptions. Industrial Health, 42(2): 252-259. https://doi.org/10.2486/indhealth.42.252
[52] Institut National de la Recherche Scientifique (INRS). (2017a). Risques chimiques. Consulted June 10, 2021. http://www.inrs.fr/risques/chimiques/mesures-hygiene.html
[53] Norheim, K.L., Bønløkke, J.H., Samani, A., Omland, Ø., Madeleine, P. (2017). The effect of aging on physical performance among elderly manual workers: protocol of a cross-sectional study. JMIR Research Protocols, 6(11): e8196. https://doi.org/10.2196/resprot.8196
[54] CPSST. (2014). Leadership. Convergence, 26(1): 1-20. https://www.centrepatronalsst.qc.ca/media/1663/conv_avril_10.pdf
[55] IRSST. (2014). Leadership. Prévention au travail, 27(2): 7-14. http://www.irsst.qc.ca/media/magazines/V27_02/7-14.pdf
[56] Salminen, S. (2004). Have young workers more injuries than older ones? An international literature review. Journal of Safety Research, 35(5): 513-521. https://doi.org/10.1016/j.jsr.2004.08.005
[57] Aubert, P., Crépon, B. (2004). Les salariés âgés sont-ils moins productifs? Gérontologie et Société, 4: 95-112.
[58] Commission des Normes, de l’équité, de la Santé et de la Sécurité du Travail. (2015). La prévention des troubles musculosquelettique. CNESST. http://www.cnesst.gouv.qc.ca/Publications/300/Documents/DC300_1002web.
[59] Heiden, B., Weigl, M., Angerer, P., Müller, A. (2013). Association of age and physical job demands with musculoskeletal disorders in nurses. Applied Ergonomics, 44(4): 652-658. https://doi.org/10.1016/j.apergo.2013.01.001
[60] Parsons, S., Breen, A., Foster, N.E., Letley, L., Pincus, T., Vogel, S., Underwood, M. (2007). Prevalence and comparative troublesomeness by age of musculoskeletal pain in different body locations. Family Practice, 24(4): 308-316. https://doi.org/10.1093/fampra/cmm027
[61] Ward, B.W., Schiller, J.S. (2013). Peer reviewed: Prevalence of multiple chronic conditions among US adults: Estimates from the National Health Interview Survey, 2010. Preventing chronic disease, 10. https://doi.org/10.5888/pcd10.120203
[62] Laville, A., Volkoff, S. (2004). 9. Vieillissement et travail. Ergonomie. Presses universitaires de France, 145-158.
[63] Quinlan, M. (1999). The implications of labour market restructuring in industrialized societies for occupational health and safety. Economic and Industrial Democracy, 20(3): 427-460. https://doi.org/10.1177/0143831x99203005
[64] Cloutier, E., Bourdouxhe, M., Ledoux, É., David, H., Gagnon, I., Ouellet, F., Teiger, C. (2005). Effets du statut d’emploi sur la santé et la sécurité au travail: le cas des auxiliaires familiales et sociales et des infirmières de soins à domicile au Québec. Perspectives Interdisciplinaires sur le Travail et la Santé, 7(2).
[65] Gonon, O. (2003). Des régulations en lien avec l’âge, la santé et les caractéristiques du travail: le cas des infirmières d’un centre hospitalier français. Perspectives interdisciplinaires sur le travail et la santé, 5(1).
[66] Chatigny, C. (2001). Les ressources de l’environnement: au cœur de la construction des savoirs professionnels en situation de travail et de la protection de la santé. Perspectives Interdisciplinaires sur le Travail et la Santé, 3(2). https://doi.org/10.4000/pistes.3719
[67] Ouellet, S., Vézina, N. (2008). Savoirs professionnels et prévention des TMS: Réflexions conceptuelles et méthodologiques menant à leur identification et à la genèse de leur construction. Perspectives interdisciplinaires sur le travail et la santé, (10-2). http://dx.doi.org/10.4000/pistes.2251
[68] Laberge, M., Tondoux, A., et Camiré Tremblay, F. (2017). Évaluation des risques liés à la SST. Les critères de conception d’un outil pour les superviseurs de stage du « Parcours de formation axée sur l’emploi. (R 968). Montréal. Institut de Recherche Robert Sauvé en santé et sécurité au Travail (IRSST). https://www.irsst.qc.ca/media/documents/PubIRSST/R-968.pdf?v=2022-10-04
[69] Sorock, G.S., Lombardi, D.A., Hauser, R.B., Eisen, E.A., Herrick, R.F., Mittleman, M.A. (2001). A case-crossover study of occupational traumatic hand injury: Methods and initial findings. American Journal of Industrial Medicine, 39(2): 171-179. https://doi.org/10.1002/1097-0274(200102)39:2%3C171::AID-AJIM1004%3E3.0.CO;2-0
[70] Van Der Beek, A.J., Kluver, B.D.R., Frings-Dresen, M.H.W., Hoozemans, M.J.M. (2000). Gender differences in exerted forces and physiological load during pushing and pulling of wheeled cages by postal workers. Ergonomics, 43(2): 269-281. https://doi.org/10.1080/001401300184602
[71] Plamondon, A., Denis, D., Larivière, C., Delisle, A., Gagnon, D., St-Vincent, M., Nastasia, I. (2012). Les femmes manutentionnaires. Un point de vue biomécanique et ergonomique. Institut de Recherche Robert-Sauvé en Santé et en Sécurité du travail (IRSST), Montreal, Quebec, Canada, 1-99.
[72] Leroy, M. (2008). Maladies professionnelles: Les femmes plus exposées. Mutualité française. https://www.mutualite.fr/actualites/maladies-professionnelles-les-femmes-plus-exposees/
[73] Serrano, N.B., Sánchez, A.S., Lasheras, F.S., Iglesias-Rodríguez, F.J., Valverde, G.F. (2020). Identification of gender differences in the factors influencing shoulders, neck and upper limb MSD by means of multivariate adaptive regression splines (MARS). Applied Ergonomics, 82: 102981. https://doi.org/10.1016/j.apergo.2019.102981
[74] Messing, K., Tissot, F., Stock, S.R. (2009). Should studies of risk factors for musculoskeletal disorders be stratified by gender? Lessons from the 1998 Quebec Health and Social Survey. Scandinavian Journal of Work, Environment & Health, 35(2): 96-112.
[75] Tissot, F., Messing, K., Stock, S. (2005). Standing, sitting and associated working conditions in the Quebec population in 1998. Ergonomics, 48(3): 249-269. https://doi.org/10.1080/00140130512331326799
[76] Too, C.L., Muhamad, N.A., Ilar, A., Padyukov, L., Alfredsson, L., Klareskog, L., MyEIRA Study Group. (2016). Occupational exposure to textile dust increases the risk of rheumatoid arthritis: Results from a Malaysian population-based case–control study. Annals of the Rheumatic Diseases, 75(6): 997-1002.
[77] Onyebeke, L.C., Papazaharias, D.M., Freund, A., Dropkin, J., McCann, M., Sanchez, S.H., Zuckerman, N.C. (2016). Access to properly fitting personal protective equipment for female construction workers. American Journal of Industrial Medicine, 59(11): 1032-1040. https://doi.org/10.1002/ajim.22624
[78] Botha, D., Cronjé, F. (2015). Occupational health and safety considerations for women employed in core mining positions. SA Journal of Human Resource Management, 13(1): 1-12. https://doi.org/10.4102/sajhrm.v13i1.652
[79] Wagner, H., Kim, A.J., Gordon, L. (2013). Relationship between personal protective equipment, self-efficacy, and job satisfaction of women in the building trades. Journal of Construction Engineering and Management, 139(10): 1-7.
[80] Vézina, M. (2011) Québec survey on working and employement conditions and occupational health and safety. (RR-707) INSPQ, Montreal. https://www.inspq.qc.ca/pdf/publications/1356_EnqQuebCondTravailEmpSanteSecTravail_VA.pdf
[81] Melamed, S., Fried, Y., Froom, P. (2004). The joint effect of noise exposure and job complexity on distress and injury risk among men and women: the cardiovascular occupational risk factors determination in Israel study. Journal of Occupational and Environmental Medicine, 1023-1032.
[82] Tomei, G., Fioravanti, M., Cerratti, D., Sancini, A., Tomao, E., Rosati, M.V., Tomei, F. (2010). Occupational exposure to noise and the cardiovascular system: a meta-analysis. Science of the Total Environment, 408(4): 681-689. https://doi.org/10.1016/j.scitotenv.2009.10.071
[83] Gan, W.Q., Davies, H.W., Demers, P.A. (2011). Exposure to occupational noise and cardiovascular disease in the United States: The National Health and Nutrition Examination Survey 1999–2004. Occupational and Environmental Medicine, 68(3): 183-190. http://dx.doi.org/10.1136/oem.2010.055269
[84] Camirand, H., Traoré, I., Baulne, J., Courtemanche, R. (2016). L'enquête québécoise sur la santé de la population 2014-2015: pour en savoir plus sur la santé des Québécois: résultats de la deuxième édition. Institut de la statistique du Québec. 2e édition, pp 189-190.
[85] Schwartz, J.B. (2003). The influence of sex on pharmacokinetics. Clinical Pharmacokinetics, 42(2): 107-121. https://doi.org/10.2165/00003088-200342020-00001
[86] Centre Canadien d’Hygiène et de sécurité au Travail. (2014). Troubles musculosquelettiques liés au travail (TMSLT). CCHST. Consulted July 4, 2021: http://www.cchst.ca/oshanswers/diseases/rmirsi.html
[87] Holizki, T., McDonald, R., Gagnon, F. (2015). Patterns of underlying causes of work-related traumatic fatalities–Comparison between small and larger companies in British Columbia. Safety Science, 71: 197-204. https://doi.org/10.1016/j.ssci.2014.06.008
[88] Hasle, P., Limborg, H.J. (2006). A review of the literature on preventive occupational health and safety activities in small enterprises. Industrial Health, 44(1): 6-12. https://doi.org/10.2486/indhealth.44.6
[89] Masi, D., Cagno, E., Micheli, G.J. (2014). Developing, implementing and evaluating OSH interventions in SMEs: A pilot, exploratory study. International Journal of Occupational Safety and Ergonomics, 20(3): 385-405. https://doi.org/10.1080/10803548.2014.11077059
[90] Toulouse, G., Nastasia, I., Imbeau, D. (2005). Étude de faisabilité en vue d’intégrer la santé et la sécurité du travail et l’ergonomie à l’approche PPA-Kaitzen. (R 428) Montréal: IRSST. Consulted July 10, 2021: https://www.irsst.qc.ca/media/documents/PubIRSST/R-428.pdf
[91] Teyssier, C. (2011). L’influence du dirigeant de SME sur les décisions financières en contexte d’hypercroissance: revue de la littérature et illustrations. Revue Internationale SME: Économie et Gestion de la Petite et Moyenne Entreprise, 24(3-4): 11-48. https://doi.org/10.7202/1013661ar
[92] CSN. (2013). LSST- Qu’est-ce que la LSST? CSN. Consulté le 05 mai 2018, tiré de: https://formationsst.csn.info/wp-content/uploads/2013/09/CSN_thematique_LSST.pdf
[93] CSN. (2014). RSST- À qui s’applique le RSST? CSN. Consulté le 05 mai 2018, tiré de : https://formationsst.csn.info/rsst/a-qui-sapplique-le-rsst/
[94] Champoux, D., Brun, J.P. (2010). Dispositions, capacités et pratiques de SST dans les petites entreprises: Opinions de Patrons, d’employés et d’intervenants en SST au Québec. Perspectives Interdisciplinaires sur le Travail et la santé, 1-21.
[95] Mendeloff, J., Gray, W.B. (2005). Inside the black box: How do OSHA inspections lead to reductions in workplace injuries? Law & Policy, 27(2): 219-237. https://doi.org/10.1111/j.1467-9930.2005.00198.x
[96] Lippel, K. (2012). Une réforme du régime québécois de santé et de sécurité : pour qui ? pourquoi ? Pour quand ? Séminaire annuel Innovations travail et emploi. Université Laval. Consulted July 9, 2021: https://www.aruc.rlt.ulaval.ca/sites/aruc.rlt.ulaval.ca/files/katherine_lippel_ppt.pdf
[97] Lamm, F. (2009). Comportement des employeurs et gestion de prévention des risques professionnels. Officiel prevention. http://www.officiel-prevention.com/protections-collectives-organisation-ergonomie/psychologie-du-travail/detail_dossier_CHSCT.php?rub=38&ssrub=163&dossid=334
[98] Amodu, T. (2008). The determinants of compliance with laws and regulations with special reference to health and safety. A literature review (Report RR-638). London School of Economics and Political Science for the Health and Safety Executive (HSE). https://www.hse.gov.uk/research/rrpdf/rr638.pdf
[99] George, K. (1985). Les comités de santé et de sécurité du travail: tables de concertation ou de négociation ? Relations Industrielles/Industrial Relations, 40(3): 512-528. https://doi.org/10.7202/050158ar
[100] Yassi, A., Lockhart, K., Sykes, M., Buck, B., Stime, B., Spiegel, J.M. (2013). Effectiveness of joint health and safety committees: A realist review. American Journal of Industrial Medicine, 56(4): 424-438. https://doi.org/10.1002/ajim.22143
[101] Commission des normes, de l’équité, de la santé et de la sécurité du travail. (2016a). Chaussures de sécurité. Consulted June 7, 2021: http://www.csst.qc.ca/prevention/theme/manutention/glossaire/Pages/chaussures_de_securite.aspx
[102] Bérubé, M. (1999). Vers un comité de santé et de sécurité efficace. (ISBN: 2-920891-58-8) Montréal, Canada, APSAM. Consulted June 16, 2021: https://www.apsam.com/sites/default/files/docs/publications/css-guide.pdf
[103] Carpentier-Roy, M.C., Ouellet, F., Simard, M., Marchand, A. (1998). Worker support for joint health and safety committees: A psychodynamic analysis. Travail Humain, 61(2): 171-185.
[104] Potvin. (2000). Le comité sst - les conditions du succès. Fiche technique # 25. APSAM. Consulted mai 6, 2018: https://www.apsam.com/sites/default/files/docs/publications/ft25.pdf
[105] Bérubé, M. (2004). Vers un comité de santé et sécurité efficace. (ISBN 978-2- 923831-0 8-4). Longueuil. Association paritaire pour la santé et la sécurité du travail du secteur de la fabrication de produits en métal, de la fabrication de produits électriques et des industries de l’habillement. Consulted mai 6, 2018: https://numerique.banq.qc.ca/patrimoine/details/52327/2024848
[106] Marchand, A., Simard, M. (1996). Les facteurs influençant l’appui des travailleurs au comité de santé-sécurité du travail. Recherches Sociographiques, 37(2): 229-246. https://doi.org/10.7202/057035ar
[107] Eaton, A.E., Nocerino, T. (2000). The effectiveness of health and safety committees: Results of a survey of public-sector workplaces the effectiveness of health and safety committees. Industrial Relations: A Journal of Economy and Society, 39(2): 265-290. https://doi.org/10.1111/0019-8676.00166
[108] Pedneault, V. (2004). Détermination des facteurs d’efficacité d’un comité de santé sécurité. M.Sc.A. inédit. Université du Québec à Chicoutimi, Québec, Canada. https://constellation.uqac.ca/640/
[109] Nichol, K., Kudla, I., Robson, L., Hon, C.Y., Eriksson, J., Holness, D.L. (2017). The develoSMEnt and testing of a tool to assess joint health and safety committee functioning and effectiveness. American Journal of Industrial Medicine, 60(4): 368-376. https://doi.org/10.1002/ajim.22703
[110] Commission des normes, de l’équité, de la santé et de la sécurité du travail. (2016b). Guide de la prévention en milieu de travail à l’intention de la petite et de la moyenne entreprise. (2e éd): Montréal, Canada: CNESST.
[111] Eckerl, G. (2014). Le programme de prévention, un outil méconnu. Prévention au travail. Consulted August 2, 2021: http://preventionautravail.com/reportages/134-le-programme-de-prevention-un-outil-meconnu.html
[112] Direction de la santé des personnes au travail. (2013). Santé et sécurité du travail. Guide pour élaborer un programme de prévention. Gouvernement du Québec. 40 p. Consulted May 4, 2021: https://www.tresor.gouv.qc.ca/fileadmin/PDF/publications/guide_programme_prevention.pdf
[113] Santos, G., Barros, S., Mendes, F., Lopes, N. (2013). The main benefits associated with health and safety management systems certification in Portuguese small and medium enterprises post quality management system certification. Safety Science, 51(1): 29-36. https://doi.org/10.1016/j.ssci.2012.06.014
[114] Organisation internationale du travail. (2011). Système de gestion en SST: Un outil pour une amélioration continue. Journée mondiale de la sécurité et de la santé au travail. (ISBN 978-92-2-224740-0) Geneva: OIT.
[115] Mohammadfam, I., Kamalinia, M., Momeni, M., Golmohammadi, R., Hamidi, Y., Soltanian, A. (2017). Evaluation of the quality of occupational health and safety management systems based on key performance indicators in certified organizations. Safety and Health at Work, 8(2): 156-161. https://doi.org/10.1016/j.shaw.2016.09.001
[116] Granerud, R.L., Rocha, R.S. (2011). Organisational learning and continuous improvement of health and safety in certified manufacturers. Safety Science, 49(7): 1030-1039. https://doi.org/10.1016/j.ssci.2011.01.009
[117] Poulin, P., Bouchard, S. (2008). L’efficience d’un système de gestion de la prévention Objectif prévention. 31(4): 11-13. https://formationsst.csn.info/wpcontent/uploads/2013/10/ASSTSAS_Efficience.pdf?toolbar=1&vi
[118] International Organization for Standardization. (2015). Santé et sécurité au travail (45 001). Genève: Organisation international de normalisation. https://www.iso.org/files/live/sites/isoorg/files/store/fr/PUB100427_fr.pdf
[119] Vinel, M. (2011). Le système de management par étapes appliqué à une SME. (M.Sc.A. inédit., Conservatoire national des arts et métiers. Institut d’Hygiène Industrielle et de l’Environnement, Paris, France). https://dumas.ccsd.cnrs.fr/dumas-00608615/document
[120] Courdeau, D., Gey, J.M. (2015). Le management de la santé et de la sécurité au travail: Maîtriser et mettre en oeuvre l'OHSAS 18001. AFNOR.Paris., 4-15.
[121] Poulin, P. (2014). Un système de gestion de la santé et de la sécurité du travail (SGSST). Webinaire. Association paritaire pour la santé et la sécurité du travail du secteur affaires sociales (ASSTSAS). http://asstsas.qc.ca/sites/default/files/publications/documents/Mat_Pedagogique/Webinaire_2014_007_SGSST_Ppants.pdf
[122] Lacasse, A., Matton, N. (2016). La santé et la sécurité du travail, il faut s’en occuper… Oui, mais comment ? P’tit Rendez-vous en santé et sécurité du travail (SST) ! Montréal: CNESST.
[123] MacEachen, E., Kosny, A., Scott-Dixon, K., Facey, M., Chambers, L., Breslin, C., Mahood, Q. (2010). Workplace health understandings and processes in small businesses: A systematic review of the qualitative literature. Journal of Occupational Rehabilitation, 20(2): 180-198. https://doi.org/10.1007/s10926-009-9227-7
[124] Ivanaj, V., Géhin, S. (1997). Les valeurs du dirigeant et la croissance de la SME. Revue internationale SME: Économie et gestion de la petite et moyenne entreprise, 10(3-4): 81-108.
[125] Champoux, D., Brun, J.P. (2015). OSH practices and interventions in small businesses: global issues in the Québec context. Policy and Practice in Health and Safety, 13(1): 47-64. https://doi.org/10.1080/14774003.2015.11667811
[126] Labelle, F., Pichette, A.M. (2016). Vigie-PME, une plateforme de transfert des connaissances dans le domaine du développement durable. Revue internationale PME, 29(3-4): 17-26. https://doi.org/10.7202/1038330ar
[127] Commission des normes, de l’équité, de la santé et de la sécurité du travail. (2011). Rôle et fonctions du comité de santé et de sécurité (CSS). CNESST. http://www.cnesst.gouv.qc.ca/Publications/1000/Documents/DC_1000_107web.pdf
[128] Constant, L. (2014). Investir en gestion de la santé et la sécurité au travail, est-ce rentable ? Forum 2014 sur la santé et sécurité du travail, pp. 33-34.
[129] Gravel, S., Lippel, K., Vergara, D., Dubé, J., Ducharme, J.F., Legendre, G. (2017). Adapter les mesures préventives de santé et de sécurité pour les travailleurs qui cumulent des précarités: les obligations d’équité. Perspectives interdisciplinaires sur le travail et la santé. (19-2). http://dx.doi.org/ 10.4000/pistes.5165
[130] Premji, S., Duguay, P., Messing, K., Lippel, K. (2010). Are immigrants, ethnic and linguistic minorities over-represented in jobs with a high level of compensated risk? Results from a Montréal, Canada study using census and workers' compensation data. American Journal of Industrial Medicine, 53(9): 875-885. https://doi.org/10.1002/ajim.20845
[131] Commission des normes, de l’équité, de la santé et de la sécurité du travail et Institut de recherche Robert-Sauvé en santé et en Sécurité du travail. (2008). Travailleurs immigrants et SST. Un nouveau contient à découvrir. Prévention au travail, (21) 7-1.
[132] Montreuil, S., Lacomblez, M., Baril-Gingras, G. (2013). La formation comme moyen d’intervention en prévention dans le domaine de la santé et de la sécurité du travail. L’intervention en santé et en sécurité du travail — Pour agir en prévention dans les milieux de travail. Presses de l’Université Laval.
[133] Baril-Gingras, G., Bellemare, M., Brun, J.P. (2007). Conditions et processus menant à des changements à la suite d’interventions en santé et sécurité du travail: l’exemple d’activité de formation ? Perspectives interdisciplinaires sur le travail et la santé, (9-1). http://dx.doi.org/10.4000/pistes.2998
[134] Robson, L.S., Clarke, J.A., Cullen, K., Bielecky, A., Severin, C., Bigelow, P.L., Mahood, Q. (2007). The effectiveness of occupational health and safety management system interventions: A systematic review. Safety Science, 45(3): 329-353. https://doi.org/10.1016/j.ssci.2006.07.003
[135] Sinclair, R., Cunningham, T.R. (2014). Predictors of safety activities in small firms. Safety Science, 64: 32-38.
[136] Freitas, A.C., Silva, S.A. (2017). Exploring OHS trainers’ role in the transfer of training. Safety Science, 91: 310-319. https://doi.org/10.1016/j.ssci.2016.08.007
[137] Konijn, A.M., Lay, A.M., Boot, C.R., Smith, P.M. (2018). The effect of active and passive occupational health and safety (OHS) training on OHS awareness and empowerment to participate in injury prevention among workers in Ontario and British Columbia (Canada). Safety Science, 108: 286-291. https://doi.org/10.1016/j.ssci.2017.12.026
[138] Silaparasetti, V., Rao, G.V.R., Khan, F.R. (2017). Social enrepreneurship: impact of occupational health and safety (OHS) factors on workers’ behavior in different construction sectors in Oman. International Journal of Management, Innovation & Entrepreneurial Research eISSN, 2395-7662.
[139] Ford, J., Henderson, R., O'Hare, D. (2014). The effects of Crew Resource Management (CRM) training on flight attendants' safety attitudes. Journal of Safety Research, 48: 49-56. https://doi.org/10.1016/j.jsr.2013.11.003
[140] Ricci, F., Chiesi, A., Bisio, C., Panari, C., Pelosi, A. (2016). Effectiveness of occupational health and safety training: A systematic review with meta-analysis. Journal of Workplace Learning.
[141] Burke, M.J., Holman, D., Birdi, K. (2006). A walk on the safe side: The implications of learning theory for developing effective safety and health training. International Review of Industrial and Organizational Psychology, 21: 1-44. https://psycnet.apa.org/doi/10.1002/9780470696378.ch1
[142] Ghosh, P., Satyawadi, R., Joshi, J.P., Ranjan, R., Singh, P. (2012). Towards more effective training programmes: A study of trainer attributes. Industrial and Commercial Training, 44(4): 191-202. https://doi.org/10.1108/00197851211231469
[143] Cohen, A., Colligan, M. (1998). Assessing occupational safety and health training: A literature review. DHSS (NIOHS) N 98-145: 11-15. https://stacks.cdc.gov/view/cdc/11254
[144] Gaudart, C., Delgoulet, C., Chassaing, K. (2008). La fidélisation de nouveaux dans une entreprise du BTP. Approche ergonomique des enjeux et des déterminants. Activités, 5(5-2). Consulted April 5, 2018: https://journals.openedition.org/activites/2013
[145] Arocena, P., Núñez, I. (2010). An empirical analysis of the effectiveness of occupational health and safety management systems in SMEs. International Small Business Journal, 28(4): 398-419. https://doi.org/10.1177/0266242610363521
[146] Kotey, B., Folker, C. (2007). Employee training in SMEs: Effect of size and firm type—Family and nonfamily. Journal of Small Business Management, 45(2): 214-238. https://doi.org/10.1111/j.1540-627X.2007.00210.x
[147] APSAM. (2018). Inspection en milieu de travail. APSAM. Consulted April 5, 2018 : https://www.apsam.com/theme/gestion/identification-des-risques/inspection-en-milieu-de-travail
[148] Eakin, J.M., Champoux, D., MacEachen, E. (2010). Health and safety in small workplaces: Refocusing upstream. Canadian Journal of Public Health, 101(1): S29-S33. https://doi.org/10.1007/BF03403843
[149] Service public fédéral, emploi, travail et concertation sociale (year) Mesures relatives à la surveillance de la santé des travailleurs. SPFETCS. Consulted June 16, 2021: http://www.emploi.belgique.be/defaultTab.aspx?id=562
[150] Guenzi, C. (2010). Visites médicales d’embauche et de reprise du travail. Tissot éditions. Consulted May 18, 2018: https://www.editions-tissot.fr/actualite/sante-securite/visites-medicales-d-embauche-et-de-reprise-du-travail
[151] Institut national de la recherche scientifique (INRS). (2017b). Prévention des risques chimiques et biologiques. INRS. Consulted June 10, 2021: http://www.irsst.qc.ca/recherche-sst/priorites-recherche/prevention-risques-chimiques-biologiques
[152] Guenzi, C. (2011). Surveillance Médicale Renforcée. Tissot éditions. Consulted May 18, 2018: https://www.editions-tissot.fr/actualite/sante-securite/surveillance-medicale-renforcee
[153] Organisation du travail. SES webclass. Consulted May 18, 2018: https://ses.webclass.fr/notions/organisation-du-travail/
[154] Organisation de travail. INRS. Consulted May 18, 2018: https://www.inrs.fr/risques/organisation/ce-qu-il-faut-retenir.html
[155] Allard, F. (2017). Organisation du temps de travail: Un temps de pause rémunéré n’est pas un avantage individuel. Tissot éditions. Consulted May 18, 2018: https://www.editions-tissot.fr/actualite/droit-du-travail/organisation-du-temps-de-travail-un-temps-de-pause-remunere-n-est-pas-un-avantage-individuel
[156] Guvin, F. (2017). Les troubles musculosquelettiques: êtes-vous concerné? Centre patronal de santé et sécurité du travail du Québec. Convergence, 33(1): 12-13. https://www.centrepatronalsst.qc.ca/media/1344/p-12-13_conv_avril_17.pdf
[157] Champoux, D., Brun, J.P. (2000). Prise en charge de la sécurité dans les petites entreprises manufacturières: état de la situation et pistes pour l’intervention et la recherche. Perspectives interdisciplinaires sur le travail et la santé. http://dx.doi.org/10.4000/pistes.3812
[158] Immigrant Québec. (2016). Travailler au Québec: Le guide pour les immigrants. Immigrant Québec. https://immigrantquebec.com/fr/consulter/guides/travailler-au-quebec
[159] Vézina, M., Cloutier, E., Stock, S., Lippel, K., Fortin, E., Delisle, A., St-Vincent, M., Funes, A., Duguay, P., Vézina, S., Prud’homme, P. (2011). Enquête québécoise sur des conditions de travail, d’emploi, et de santé et de sécurité du travail (EQCOTESST), Québec, Institut de recherche Robert-Sauvé en santé et sécurité du travail (IRSST) - Institut national de santé publique du Québec (INSPQ) et Institut de la statistique du Québec. (RAPPORT R-691). http://www.irsst.qc.ca/media/documents/pubirsst/r-691.pdf
[160] Sparks, K., Cooper, C., Fried, Y., Shirom, A. (1997). The effects of hours of work on health: a meta‐analytic review. Journal of Occupational and Organizational Psychology, 70(4): 391-408.
[161] Ruta, S., Dagenais, L.F. (2003). Travail en transition, santé mentale et conditions de travail: Rapport de recension documentaire (phase I) et proposition de recherche (phase II). Commission des droits de la personne et des droits de la jeunesse. https://numerique.banq.qc.ca/patrimoine/details/52327/1904369
[162] Boyd, C. (2004). Human resource management and occupational health and safety. Routledge.
[163] Gollac, M., Volkoff, S. (2006). La santé au travail et ses masques. Actes de la recherche en sciences sociales, (3): 4-17. https://doi.org/10.3917/arss.163.0004
[164] Edouard, F. (2010). Le travail de nuit : impact sur les conditions de travail et de vie des salariés. (X10000112V). Conseil économique, social et environnemental. https://www.lecese.fr/travaux-publies/le-travail-de-nuit-impact-sur-les-conditions-de-travail-et-de-vie-des-salaries
[165] Lippel, K., Johnstone, R., Baril-Gingras, G. (2017). Introduction: Regulation, Change and the Work Environment/Introduction: Régulation, changement et environnement du travail. Relations industrielles/Industrial Relations, 72(1): 3-32. https://www.proquest.com/docview/2714154726/F85D84DFCBB7471BPQ/1?accountid=13835
[166] Mayhew, C., Quintan, M., Ferris, R. (1997). The effects of subcontracting/outsourcing on occupational health and safety: Survey evidence from four Australian industries. Safety Science, 25(1-3): 163-178. https://doi.org/10.1016/S0925-7535(97)00014-3
[167] Quinlan, M., Thébaud-Mony, A. (2009). La sous-traitance et la SST dans les petites entreprises: une relation négligée. Officiel prévention. http://www.officielprevention.com/formation/conseils/detail_dossier_CHSCT.php?rub=89&ssrub=183&dossid=333
[168] Rachid Belkacem et Laurence Montcharmont. (2012). Analyse des conditions de travail des travailleurs intérimaires . Perspectives interdisciplinaires sur le travail et la santé, (9-1). http://dx.doi.org/10.4000/pistes.2543
[169] Officiel prévention. (2014). La prévention des risques professionnels des intérimaires. Consulted June 3, 2018: https://www.officiel-prevention.com/dossier/formation/fiches-metier/la-prevention-des-risques-professionnels-des-interimaires
[170] Champoux, D., Prud’homme, P. (2017). Analyse comparative du contexte de travail et portrait statistique des problèmes de santé et sécurité au travail en fonction de la taille des entreprises. (R-986). IRSST. https://www.irsst.qc.ca/media/documents/PubIRSST/
[171] Simard, M., Marchand, A. (1997). La participation des travailleurs à la prévention des accidents du travail: formes, efficacité et déterminants. Institut de recherche en santé et en sécurité du travail du Québec, 47.
[172] Gravel, S., Lippel, K., Vergara, D., Dubé, J., Ducharme, J.F., Legendre, G. (2017). Adapter les mesures préventives de santé et de sécurité pour les travailleurs qui cumulent des précarités: les obligations d’équité. Perspectives interdisciplinaires sur le travail et la santé. (19-2). http://dx.doi.org/ 10.4000/pistes.5165
[173] Hämmig, O. (2017). Health and well-being at work: The key role of supervisor support. SSM-Population Health, 3: 393-402. https://doi.org/10.1016/j.ssmph.2017.04.002
[174] Willemse, B.M., de Jonge, J., Smit, D., Depla, M.F., Pot, A.M. (2012). The moderating role of decision authority and coworker-and supervisor support on the impact of job demands in nursing homes: A cross-sectional study. International Journal of Nursing Studies, 49(7): 822-833. https://doi.org/10.1016/j.ijnurstu.2012.02.003
[175] Petit, A., Roquelaure, Y. (2014). Pathologie discale et maladie professionnelle. Revue du Rhumatisme Monographies, 81(1): 52-56. https://doi.org/10.1016/j.monrhu.2013.11.001
[176] Richomme-Huet, K., d’Andria, A. (2010). Interactions entre les pratiques de ressources humaines et intrapreneuriales en SME. Management Avenir, (9): 136-148.
[177] Marlow, S., Patton, D. (1993). Managing the employment relationship in the smaller firm: Possibilities for human resource management. International Small Business Journal, 11(4): 57-64. https://doi.org/10.1177/026624269301100404
[178] Marlow, S., Patton, D. (2002). Minding the gap between employers and employees: The challenge for owner‐managers of smaller manufacturing firms. Employee Relations, 24(5): 523-539. https://doi.org/10.1108/01425450210443294
[179] Walters, D., Lamn, F. (2003). OHS in small organisations: Some challenges and ways forward. In Australian OHS regulation for the 21st century. Nationalresearch centre for occupational health and safety regulation & national occupational health and safety commission, Gold Coast. https://openresearch-repository.anu.edu.au/bitstream/1885/41224/3/WP15.Lammandwalters.pdf
[180] Caisse d’assurance retraite et de la santé au travail CARSAT. (2013). Management de la Santé et de la Sécurité au Travail retours d’expériences. Un guide pratique à l’usage des PME. Retraite et santé au travail. Aquitaine, Franc.
[181] Kaassis, B., Badri, A. (2018). DeveloSMEnt of a preliminary model for evaluating occupational health and safety risk management maturity in small and medium-sized enterprises. Safety, 4(1): 5. https://doi.org/10.3390/safety4010005
[182] Bonafede, M., Corfiati, M., Gagliardi, D., Boccuni, F., Ronchetti, M., Valenti, A., Iavicoli, S. (2016). OHS management and employers’ perception: Differences by firm size in a large Italian company survey. Safety Science, 89: 11-18. https://doi.org/10.1016/j.ssci.2016.05.012
[183] Reinhold, K., Järvis, M., Tint, P. (2015). Practical tool and procedure for workplace risk assessment: Evidence from SMEs in Estonia. Safety Science, 71: 282-291. https://doi.org/10.1016/j.ssci.2014.09.016
[184] Boustras, G., Guldenmund, F.W. (2017). Safety management in small and medium-sized enterprises (SMEs). CRC Press.
[185] Fédération régionale des SSTI des Pays de la Loire. (2013). Guide pratique. D’évaluation et de prévention du risque chimique en entreprise edition 2013.Présanse Pyas de la Loire. https://www.risquechimiquepaysdelaloire.org/sites/default/files/guide_pratique_risque_chimique_ssti_pays_de_la_loire_-_edition_2013.pdf
[186] Laird, I., Olsen, K., Harris, L.A., Legg, S., Perry, M.J. (2011). Utilising the characteristics of small enterprises to assist in managing hazardous substances in the workplace. International Journal of Workplace Health Management, 4(2): 140-163. https://doi.org/10.1108/17538351111143312
[187] Coutrot, T., Léonard, M. (2017). Les expositions aux risques professionnels dans les petits établissements en 2010. Références en santé au travail, 152: 75-85.
[188] Walters, D. (2006). The efficacy of strategies for chemical risk management in small enterprises in Europe: Evidence for success? Policy and Practice in Health and Safety, 4(1): 81-116. https://doi.org/10.1080/14774003.2006.11667677
[189] Terwoert, J., Verbist, K., Heussen, H. (2016). An intervention study on the implementation of control banding in controlling exposure to hazardous chemicals in small and medium-sized enterprises. Safety and Health at Work, 7(3): 185-193. https://doi.org/10.1016/j.shaw.2015.12.002
[190] Diallo, F. (2008). Outils d'aide à la substitution des substances toxiques hors solvants 30 e Congrès de l’AQHSST. Laval: AQHSST. http://www.congresaqhsst.ca/archives-congres/2006-2010/
[191] Balty et Chapouthier. (2013). Les équipements de protection individuels. Règle d’utilisation (ED 6077). Paris: INRS. www.inrs.fr/dms/inrs/CataloguePapier/ED/TI-ED-6077/ed6077.pdf
[192] Boutin, J. (2008). Prévention Santé Environnement. Academie de noramndie, Sicences biologiques et sicences socilaes. https://sbssa.ac-normandie.fr/prevrisquemvm
[193] Oksel, C., Subramanian, V., Semenzin, E., Ma, C.Y., Hristozov, D., Wang, X.Z., Neil Hunt, N., Costa, A., Fransman, W., Marcomini, A., Wilkins, T. (2016). Evaluation of existing control measures in reducing health and safety risks of engineered nanomaterials. Environmental Science: Nano, 3(4): 869-882. https://doi.org/10.1039/C6EN00122J
[194] Fabiano, B., Currò, F., Pastorino, R. (2004). A study of the relationship between occupational injuries and firm size and type in the Italian industry. Safety Science, 42(7): 587-600. https://doi.org/10.1016/j.ssci.2003.09.003
[195] INRS. (2009). Les équipements de protection des yeux et du visage. (ED 798). INRS. Paris. Consulted June 6, 2018: file:///G:/ed798.pdf
[196] APSAM. (2017). Équipements de protection individuels – généralités. APSAM. https://www.apsam.com/theme/moyens-et-equipements-de-protection/epi-generalites
[197] Centre Canadien d’Hygiène et de sécurité au Travail. (2017). Protection des machines. CCHST. https://www.cchst.ca/products/csa/27020722004/
[198] Arcury, T.A., Grzywacz, J.G., Anderson, A.M., Mora, D.C., Carrillo, L., Chen, H., Quandt, S.A. (2013). Employer, use of personal protective equipment, and work safety climate: Latino poultry processing workers. American Journal of Industrial Medicine, 56(2): 180-188. https://doi.org/10.1002/ajim.22101
[199] Floyde, A., Lawson, G., Shalloe, S., Eastgate, R., D’Cruz, M. (2013). The design and implementation of knowledge management systems and e-learning for improved occupational health and safety in small to medium sized enterprises. Safety Science, 60: 69-76. https://doi.org/10.1016/j.ssci.2013.06.012
[200] De Marcellis-Warin, N., Peignier, I., Hart, C., Warin, T. (2011). Identification des partenaires stratégiques des SME au Québec et portrait de leurs activités en lien avec l’environnement et les produits chimiques, 2011: rp-06. CIRANO.
[201] APSAM. (2006). La CSST lance la phase II du Programme intégré pour la prévention des risques biologiques. APSAM, 15(1): 10. https://www.apsam.com/sites/default/files/docs/publications/revue/vol15-no1.pdf
[202] Beaulieu, C., Marien, C., Tremblay, M. (2003). Guide de gestion des risques biologiques à l’intention des groupes visés par le programme d’intervention intégré sur les risques biologiques. CSST. 8-22. https://numerique.banq.qc.ca/patrimoine/details/52327/1983881
[203] Millette. (2014). Prévention auditive. Présentation aux collaborateurs de l’ASFETM. ASFETM. https://asfetm.com/wp-content/uploads/2013/12/PreventionauditiveCollaborateurs2014.pdf
[204] Lebeau, M., Duguay, P. (2011). Les coûts des lésions professionnelles: une revue de littérature (R 676) Montréal: IRSST. https://www.irsst.qc.ca/media/documents/PubIRSST/R-676.pdf?v=2019-06-21
[205] Girard, S.A., Leroux, T., Verreault, R., Courteau, M., Picard, M., Turcotte, F., Richer, O. (2015). Cardiovascular disease mortality among retired workers chronically exposed to intense occupational noise. International Archives of Occupational and Environmental Health, 88(1): 123-130. https://doi.org/10.1007/s00420-014-0943-8
[206] OIT. (2018). C148 - Convention (n° 148) sur le milieu de travail (pollution de l'air, bruit et vibrations). OIT. https://www.ilo.org/dyn/normlex/fr/f?p=NORMLEXPUB:13100:0::NO::P13100_COMMENT_ID:3960997
[207] Buissonnet, S. (2007). Le bruit en limieu du travail. Toujours présent.Parlsons-en ! Le boulot santé. https://www.santeautravail.qc.ca/c/document_library/get_file?uuid=aa882545-a1c7-4ca5-8516-64b79222b5c1&groupId=67467
[208] Nguyen, P., Parent, G. (1998). Réduire le bruit en milieu de travail Informations générales et techniques illustrées Pour mieux s’entendre.CSST. 7-14. https://numerique.banq.qc.ca/patrimoine/details/52327/1984195?docref=3RdNn3K1TRTBcvXvGPm4bA
[209] Chambre de Commerce et d’Industrie France. (2016). Guide SME/PMI Prévention des risques santé et sécurité au travail — Responsabilité sociétale de l’entreprise, pp. 37-41.
[210] Singh, L.P., Bhardwaj, A., Deepak, K.K. (2010). Occupational exposure in small and medium scale industry with specific reference to heat and noise. Noise and Health, 12(46): 37.
[211] Guo, J., Gunn, P. (2004). Occupational noise control in Australia- Its policy and management. Canadian Acoustics, 32(4).
[212] Suter, A.H. (2012). Engineering controls for occupational noise exposure. Sound and Vibration, 46: 24-31.
[213] Hohmann, B.W. (2008). Simple evaluation of occupational noise exposure without measurements. Journal of the Acoustical Society of America, 123(5): 3527.
[214] Ministère du travail ontarien. (2009). Rayonnement ultraviolet dans les lieu de travail. Ministère du travail ontario. https://www.publications.gov.on.ca/browse-catalogues/occupational-health-safety/health-safety-guidelines/rayonnement-ultraviolet-dans-les-lieu-de-travail-mars-2009
[215] Camirand and Berthelot. (2017). Les Québécois âgés de 15 à 29 ans sont-ils plus exposés aux contraintes physiques en milieu de travail que leurs aînés? Des résultats tirés de l’Enquête québécoise sur la santé de la population, 2014-2015. Institut de la Statistique du Québec. Zoom Santé, 64. https://statistique.quebec.ca/fr/fichier/no-64-les-quebecois-ages-de-15-a-29-ans-sont-
[216] Lachance, N., Caron, S. (2016). Travailleurs… Attention aux vibrations, il y a des effets sur la santé ! Centre integré et des services sociaux de la Côte-Nord, 23(3). https://www.cisss-cotenord.gouv.qc.ca/fileadmin/internet/cisss-cotenord/Documentation/Bulletins_sante_publique/Sante_en_tetes/Vol._23__no_3_-
[217] Poirier-Lavallée, M. ( 2016 ). Vibrations en milieu de travail. Santé en tête. Centre integré et des services sociaux de la Côte-Nord, 23(3). https://www.cisss-cotenord.gouv.qc.ca/fileadmin/internet/cisss-cotenord/Documentation/Bulletins_sante_publique/Sante_en_tetes/Vol._23__no_3
[218] Giorgio, M.T. (2018). Vibrations mécaniques: réglementation. Atousanté. https://www.atousante.com/risques-professionnels/risques-physiques/vibrations-mecaniques/vibrations-mecaniques-reglementation/
[219] Turcot, A., Dumitrescu, M., Fortier, M., Marcotte, P., Bernier, V. (2016). Caractérisation du syndrome du marteau hypothénarien chez les travailleurs utilisant des outils manuels et exposés aux vibrations main-bras. INSPQ. https://numerique.banq.qc.ca/patrimoine/details/52327/2754135
[220] Gervais, M., Massicotte, P., Champoux, D. (2006). Conditions de travail, de santé et de sécurité des travailleurs du Québec (R449). Montréal, Canada: IRSST.
[221] Commission des normes, de l’équité, de la santé et de la sécurité du travail. (2017). Ce que vous devez savoir sur les mutuelles de prévention. http://www.cnesst.gouv.qc.ca/Publications/200/Documents/DC200-1434web.pdf
[222] Institut national de la recherche scientifique (INRS). (2014). Protection collective. http://www.inrs.fr/demarche/protection-collective/ce-qu-il-faut-retenir.html
[223] Danzl, D.F. (2018). Présentation des lésions provoquées par le froid. Le manuel merck. https://www.merckmanuals.com/fr-ca/accueil/l%C3%A9sions-et-intoxications/l%C3%A9sions-provoqu%C3%A9es-par-le-froid/gelure
[224] Vidal-Léon, I. (2015). La chaleur et le froid au travail. Osez vos devoir. https://www.osezvosdroits.com/la-chaleur-et-le-froid-au-travail/
[225] Ménard, L. (2009). Guide de prévention pour l'assainissement des systèmes de chauffage, de ventilation et de conditionnement de l'air. CSST. https://www.cnesst.gouv.qc.ca/sites/default/files/publications/guide-assainissement-systemes-chauffage-ventilation-conditionnement-lair.pdf
[226] Vega, P. ( 2016). Prévention des risques électriques. 16 eme Grand Rendez-vous en santé et sécurité Montréal. ASFETM. http://asfetm.com/wp-content/uploads/2013/11/GRV-1er-novembre-2016-Risques-%C3%A9lectriques-Web1.pdf
[227] Bourgeois, F., Hubault, F. (2005). Prévenir les TMS. De la biomécanique à la revalorisation du travail, l’analyse du geste dans toutes ses dimensions. Activités, 2(2-1). https://journals.openedition.org/activites/1561
[228] Bellemare, M., Montreuil, S., Marier, M., Prévost, J., Allard, D. (2001). L’amélioration des situations de travail par l’ergonomie participative et la formation. Relations Industrielles/Industrial Relations, 56(3): 470-490.
[229] Falzon, P. (2014). Constructive ergonomics. In Fabien, C. and Johann P., Prevention of MSDs and the development of empowerme (1er Edition. 171). Boca Roton: CRC Press. https://doi.org/10.1201/b17456
[230] Lippel, K. (2009). Le droit québécois et les troubles musculo-squelettiques: Règles relatives à l’indemnisation et à la prévention. Perspectives interdisciplinaires sur le travail et la santé. http://dx.doi.org/10.4000/pistes.2381
[231] Gauvin, F. (2018). Les troubles musculosquelettiques : êtes-vous concerné? Centre patronal de santé et sécurité du travail du Québec. Convergence: 12-13. https://www.centrepatronalsst.qc.ca/media/1344/p-12-13_conv_avril_17.pdf
[232] Denis, D., St-Vincent, M., Imbeau, D., Jetté, C., Nastasia, I. (2008). Intervention practices in musculoskeletal disorder prevention: A critical literature review. Applied Ergonomics, 39(1): 1-14.
[233] Hemphälä, H., Eklund, J. (2012). A visual ergonomics intervention in mail sorting facilities: effects on eyes, muscles and productivity. Applied Ergonomics, 43(1): 217-229.
[234] Simoneau, S., St-Vincent, M., Chicoine, D. (2013). Les TMS des membres supérieurs: mieux les comprendre pour mieux les prévenir. IRSST. http://www.irsst.qc.ca/media/documents/PubIRSST/RG-779.pdf
[235] St-Jacques, Y., Ross, M.J. (2018). TMS - Idées de prévention pour les meuleurs et les polisseurs. Multiprévention. https://multiprevention.org/wp-content/uploads/2016/07/multiprevention-guide-meuleurs-polisseurs.pdf
[236] Thibault, J.F., Merlin, X., Garrigou, A. (2013). De la production à l’usage de la mesure, quelle appropriation par deux entreprises industrielles? Pour quelle prévention des TMS?. Perspectives interdisciplinaires sur le travail et la santé, (15-2). https://journals.openedition.org/pistes/3430?lang=en
[237] Malchaire, J. (2002) Stratégie générale de gestion des risques professionnels. Illustration dans le cas des ambiances thermiques au travail. INRS, 186: 39-49. www.inrs.fr/dms/inrs/CataloguePapier/ND/TI-ND-2165/nd2165.pdf
[238] Teiger, C. (2002). Origines et évolution de la formation à la prévention des risques « gestes et postures » en France. Relations Industrielles/Industrial Relations, 57(3): 431-462.
[239] Robson, L.S., Stephenson, C.M., Schulte, P.A., Amick III, B.C., Irvin, E.L., Eggerth, D.E., Peters, R.H. (2012). A systematic review of the effectiveness of occupational health and safety training. Scandinavian Journal of Work, Environment & Health, 193-208.
[240] Teiger, C., Montreuil, S. (1996). The foundations and contributions of ergonomics work analysis in training programmes. Safety Science, 23(2): 81-95.
[241] Guimarães, L.D.M., Anzanello, M.J., Renner, J.S. (2012). A learning curve-based method to implement multifunctional work teams in the Brazilian footwear sector. Applied Ergonomics, 43(3): 541-547. https://doi.org/10.1016/j.apergo.2011.08.008
[242] Faucher, M.L. (2004). Est-ce une solution ? La rotation des potes de travail. IRSST. http://www.irsst.qc.ca/media/magazines/v17_02/37-39.pdf
[243] Lanouzière, H. (2015). La définition du travail répétitif comme facteur de pénibilité. Rapport aux Ministres : des affaires sociales, de la santé et des droits des femmes - du travail, de l’emploi, de la formation professionnelle et du dialogue social. Vie publique. https://www.vie-publique.fr/rapport/35205-la-definition-du-travail-repetitif-comme-facteur-de-penibilite