Alfonsus H. Harianja*![]() | Haryoto Kusnoputranto
| Haryoto Kusnoputranto![]() | Tri Edhi Budhi Soesilo
| Tri Edhi Budhi Soesilo![]()
© 2025 The authors. This article is published by IIETA and is licensed under the CC BY 4.0 license (http://creativecommons.org/licenses/by/4.0/).
OPEN ACCESS
The presence of artisanal and small-scale gold mining (ASGM) in Indonesia has led to adverse environmental and human health impacts due to the use of mercury in ore processing. Unlike previous similar studies on ASGM in Indonesia, this study employed a quantitative approach involving a larger and more representative group of participants. It combined hair and urine biomarkers according to exposure pathways to analyze individuals' total mercury exposure. This study applied a health-related quality of life (HRQoL) assessment using the EQ-5D-5L and VAS instruments for the first time in the Indonesian ASGM population. Additionally, it examined the correlation between socio-economic factors and mercury exposure. The study was carried out in three ASGM sites in Ciemas, Waluran, and Lengkong subdistricts, Sukabumi Regency, from October 2023 to August 2024. This research determined the sample size (n = 400) through simple random sampling using the Slovin formula at a 95% confidence level. The results showed the average mercury level in hair was 1.67 µg/g, with 43.5% of respondents in the “alert” to “high” categories based on WHO reference values. In urine, the average level reached 35.81 µg/L, with 74.75% of respondents exceeding the HBM2 reference values. No significant difference was found between miners and non-miners, indicating widespread environmental exposure. In addition, the standardized HRQoL instruments showed that while over 72% of respondents rated their health as good, at least 30% reported physical discomfort, and 20% experienced emotional issues. A more in-depth health assessment also revealed that respondents experienced several symptoms or health issues consistent with mercury toxicity, including muscle cramps, headaches, respiratory problems, and internal organ disorders. Correlation analysis revealed a weak but significant association between monthly income and mercury levels in hair. Among miners, longer work duration also correlated significantly with higher mercury exposure. The findings underscore the need for comprehensive interventions that target both environmental control and community health protection in ASGM area.
artisanal and small-scale gold mining, environment, mercury, hair, heath-related quality of life, socio-economic, urine
Artisanal and small-scale gold mining (ASGM) in Indonesia has existed since the colonial era and has developed widely across almost all regions. The existence of traditional gold mining (PESK) in various locations across Indonesia generally develops by following the pattern of large-scale gold mining operations in the region, such as Freeport in Papua, Amman Mineral in Nusa Tenggara, Martabe and Sorik Mas Mining in North Sumatra, Antam in Banten, and Bumi Resources Minerals in Poboya, Central Sulawesi Provinces. ASGM has been operating in 30 provinces across Indonesia in 2020, according to the Ministry of Environment and Forestry of the Republic of Indonesia. The four provinces that do not have ASGM are the Riau Islands, Bangka-Belitung, DKI Jakarta, and Bali. The highest number of miners is found in Central Kalimantan Province, it is 24,500 individuals, while the lowest numbers are in North Maluku and West Papua Provinces, with 500 miners respectively. In total, the data reported that the active miner in Indonesia in 2020 was 169,325 individuals.
However, since ASGM in Indonesia is generally still illegal and traditional, the workforce tends to move easily in and out of the sector, making it challenging to provide an accurate count of miners [1]. One source estimates that the number of ASGM miners is even higher, reaching approximately 250,000 individuals in 2011, with a positive growth trend [2], and supporting the livelihoods of around 2 million people [3].
Community involvement in ASGM has been highlighted in previous studies [4, 5]. Several studies reported that this sector increases household income in various locations [6-8] and also contributes to rural and regional economies [9, 10]. ASGM can serve as the primary source of household income and even play a role in reducing rural poverty [6, 11]. The integration of ASGM into the regional economic system also contributes economically to nearby urban areas, such as in Tatelu, North Sulawesi [12], Mandor, West Kalimantan [13], Poboya, Central Sulawesi [2], and Makassar, South Sulawesi [14].
Earlier studies have documented the environmental impacts of mercury use in gold ore processing of ASGM in Indonesia, including measurements of contamination across various environmental media and human exposure levels. Mercury pollution has been detected in water bodies [15], soil and plants [16-18], biota such as fish and mammals [19-21], and in humans, both miners [22-24] and nonminers living nearby mining areas [23].
Other studies have attempted to identify socioeconomic factors associated with mercury contamination in the environment and human exposure. Demographic factors, including gender, length of residence, and employment status, are significant in ASGM [25-27]. In addition, social factors such as knowledge, perception, community values, and levels of participation influence public awareness and attitudes toward environmental pollution control [28-30]. Socio economic dynamics are also shaped by the roles of stakeholders, including governance, legal frameworks, and institutional capacity at both local and national levels [31-33].
Indonesia's policy to reduce mercury use in ASGM began with its participation in the Intergovernmental Negotiating Committee (INC) under the United Nations Environmental Programme (UNEP), which led to the country becoming a signatory to the Minamata Convention on Mercury. Indonesia affirmed that the research underpinning the convention applied to the national context and aligned with the government's political commitment to eliminate mercury use in ASGM.
At the national level, the government has set a target to reduce and eliminate mercury use in ASGM by 2025, by Presidential Regulation No. 21 of 2019 concerning the National Action Plan (NAP) for Mercury Reduction and Elimination. Addressing mercury contamination requires a holistic control approach that encompasses social, economic, health, and environmental aspects. Key areas for action include understanding the level of human exposure through biomarker samples, assessing public health conditions in communities near ASGM sites, analysing the correlation of socioeconomic and environmental factors, and identifying solution alternatives through comprehensive methods [34, 35].
The ASGM sector involves approximately 7,125 miners spread across Bogor, Kuningan, Tasikmalaya, and Sukabumi regencies in West Java Province. A preliminary study in Sukabumi Regency revealed that mercury usage is significantly high in ASGM operation [7]. Approximately 200 to 400 grams of mercury are used in the processing of materials to produce 0.8 to 4 grams of gold per month per mining operation, resulting in an estimated total mercury usage of 130 to 520kg per month. The release of mercury into the environment, including soil, water, air, and biota, poses a potential risk of human exposure. Controlling environmental pollution and its associated health hazards remains a critical issue that needs to be addressed, while also considering the sustainability of economic and social benefits produced.
The specific objectives of the research are to analyze the level of mercury exposure in communities around ASGM sites, to analyze the health status of the community using European Quality of Life 5 dimensions 5 level (EQ-5D-5L) of health-related quality of life (HRQoL) associated with mercury exposure, and to analyze the correlation between social and economic factors and mercury exposure.
2.1 Theoretical framework
Indonesian Law No. 32 of 2009 on Environmental Protection and Management defines environmental pollution as the entry of living organisms, substances, energy, or other components into the environment that exceeds quality standards. Similarly, Miller and Spoolman [36] define environmental pollution as the contamination of the environment by substances or energy (such as chemicals, heat, or noise) beyond acceptable thresholds, posing a threat to human health and other organism. Anthropogenic activities, particularly ASGM, are primarily responsible for mercury pollution [37]. The Minamata Convention on Mercury recognizes mercury exposure as a global priority issue affecting both human health and the environment [38].
Mercury, a toxic heavy metal, enters the air, water, and soil through both natural processes and human activities [39]. Industries use mercury in various sectors, including as an amalgamating agent in ASGM. Mercury occurs in elemental, inorganic, and organic forms. Elemental mercury readily evaporates and travels across the globe. In aquatic environments, microorganisms convert it into methylmercury, which accumulates in the food chain and poses a threat to human health.
Several studies in Indonesia have reported mercury exposure levels in populations living near ASGM sites, including in Aceh, South Sulawesi, Southeast Sulawesi, Banten, Gorontalo, and West Java Provinces. In many of these areas, exposure levels exceed mercury safety standards set by the World Health Organization (WHO) or the German Human Biomonitoring Commission (HBM). Mercury can enter the human body through two primary pathways: inhalation and ingestion of contaminated food or drink. According to Cunningham and Cunningham [40], human cells have a mechanism termed bioaccumulation, which enables them to absorb and store harmful substances, such as toxic chemicals. Through food webs, these substances can undergo biomagnification, resulting in an increase in concentration at higher trophic levels.
This study adopts the theory of environmental pollution, focusing on mercury contamination resulting from its use in gold ore processing. Based on previous research [26], the measured parameters include total mercury concentrations in human biomarkers, specifically hair and urine, of individuals living and working around ASGM sites.
Mercury has serious toxic effects on human health, particularly damaging the brain and central nervous system in both adults and vulnerable populations such as fetuses, infants, and children [41-44]. Exposure through ingestion, inhalation, or dermal contact can lead to neurological disorders, as well as impairments in the digestive, immune, respiratory, and renal systems [39, 45-47]. Common symptoms of mercury poisoning include tremors, insomnia, memory loss, cognitive and motor dysfunction, and headaches. In fetuses and children, mercury exposure may result in neurodevelopmental disorders such as intellectual disabilities, seizures, visual and auditory impairments, growth retardation, speech difficulties, and acrodynia [48-50].
A study by Steckling et al. [51] quantified the global health burden of mercury. The findings revealed the highest risks in Latin America and Africa, with moderate risk levels observed in the Sumatra, Java, and Sulawesi regions of Indonesia, and high-risk levels in Kalimantan and Papua.
This study utilizes community health status as a variable, which is constructed from the population's quality of life, determined by five factors: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression [52, 53]. It also employs the Visual Analogue Scale (VAS) to assess self-perceived health status, which is valued from 0 (worst imaginable health) to 100 (best possible health).
Several studies have demonstrated that socioeconomic factors significantly contribute to mercury exposure levels in humans. While some studies have directly examined these relationships, most have focused on the general socioeconomic characteristics of communities surrounding ASGM. Research conducted in both Africa [26] and Indonesia suggests that low public awareness [8, 38, 54] and urgent economic needs [55-57] are underlying factors that reduce concern for environmental impacts.
Moreover, the involvement of poorly educated community members in ASGM increases the risk of mercury exposure [7, 8]. A preliminary study revealed that residents in Sukabumi [7] had been exposed to mercury levels classified as "alert level" according to the WHO standards. This study uses those findings, employing larger sample sizes and additional data, to statistically examine the correlation between socioeconomic variables and mercury concentrations in the human body.
2.2 Time and location of study
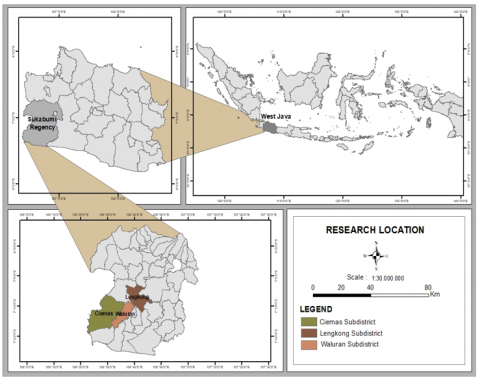
This research was conducted from November 2023 to August 2024 in ASGM areas within Sukabumi Regency, specifically in the subdistricts of Ciemas, Waluran, and Lengkong. Geographically, these subdistricts are located in the southern part of Sukabumi Regency, lying between 106o20’00”E-106o45’00”E and 7o00’00”S-7o20’00”S and some parts border directly with the Indian Ocean. Waluran is situated to the west of Ciemas, while Lengkong lies to the east of Waluran (Figure 1). All three subdistrict centers are situated more than 48 kilometers from Palabuhanratu, the capital of Sukabumi Regency, and are accessible by four-wheeled vehicles. However, some villages within these subdistricts can only be reached by two-wheeled vehicles.
Figure 1. Study area
2.3 Data collection and analysis
The data collection process included the gathering of primary data on mercury exposure through hair and urine samples, public health status, and community socioeconomic conditions. The population of this study consists of the residents of the third subdistrict who are potentially exposed to mercury. The study determines the number of respondents representing the population using simple random sampling based on the Slovin formula, where n = N/(1 + Ne2), with n representing the required sample size, N the population size, and e the margin of error, set at 5%. Based on the official 2023 population data from the Central Bureau of Statistics of Sukabumi Regency, with a 95% confidence level, the study determined that a total of 400 respondents would be included, as shown in Table 1.
Table 1. Number of research samples
|
No. |
Subdistrict |
Population |
Proportion |
Sample Size |
|
1 |
Ciemas |
56,344 |
0.46 |
185 |
|
2 |
Waluran |
31,686 |
0.26 |
104 |
|
3 |
Lengkong |
33,700 |
0.28 |
111 |
|
|
Total |
121,730 |
1 |
400 |
Respondents were selected using an accidental sampling method, with the following inclusion criteria: individuals aged 17 years or older or already married, willing to provide hair and urine samples (as confirmed by signed informed consent), and willing to be interviewed regarding their health status based on HRQoL and their socioeconomic characteristics. The School of Environmental Science, University of Indonesia's Ethics Review Committee approved this study under Number KET 036/UN2.F13.D1.KE1/PPM.00/2023, dated 11 December 2023. In addition, secondary data on environmental mercury contamination were collected to support and contextualize the primary data.
2.3.1 Mercury exposure
This research assessed mercury exposure by measuring total mercury (T-Hg) levels in the hair and urine of respondents. Hair samples were collected by cutting hair approximately 1cm from the scalp, stored them in small labeled plastic bags with the respondent's name and identification number, and kept them at room temperature for laboratory analysis. Mercury analysis in hair samples was conducted at the accredited laboratory of Center for Environmental Quality Research and Development Laboratory, Ministry of Environment and Forestry (MoEFRI) and at the National Research and Innovation Agency (BRIN), using the UNEP 7473 standard procedure.
The total mercury analyses in hair began with cleaning the hair samples using acetone, followed by deionized water, and then dried at 50℃ oven until a constant weight was achieved. The total mercury in the hair sample was determined using the open-flask method. Each weighed sample was placed into three separate boiling tubes, each containing 0.5g of hair sample, 5.0mL of sulfuric acid, and 2.0mL of a mixed solution of perchloric acid and nitrous acid (in a 1:1 ratio). Afterward, 1.0mL of deionized water was added. The tubes were then placed on a sand bath at a temperature of 200 ± 5℃ until the compounds were fully digested. The solution was then cooled to room temperature and diluted with 50mL of deionized water.
Urine samples were collected from each respondent in 100 mL plastic tubes, sealed, and placed in cold boxes for transport to laboratory for analysis. The laboratory of Provincial Health Office of DKI Jakarta analyzed the samples. In the laboratory, 20.0mL of urine was mixed with 20.0mL of an acid solution consisting of sulfuric acid, perchloric acid, and nitrous acid (in a 3:1:1 ratio). The mixture was heated at 50℃ until its volume was reduced to 20.0mL, then diluted with 50mL of deionized water to form a marker solution. Subsequently, standard mercury solutions with volumes of 100, 50, and 25µL (prepared from a one µg/mL stock solution) were made using the same procedure.
The prepared samples were then placed in glass bottles, and the total mercury concentration was analyzed using VAAS with an automatic mercury analyzer (HG 5000). Measurement quality standards were ensured by conducting quality control analyses, including sample replication, reagent blanks, and pre- and post-digestion spikes. Samples were divided according to variations in mercury (Hg) levels to verify the reliability of the analytical method and assess the stability of the recovery results. The instruments used had detection limits of 0.08 µg/g for hair and 1.20 µg/L for urine, with recovery rates exceeding 90%.
Hair serves as one of the most efficient biomarkers for measuring mercury toxicity in humans. Hair mercury content reflects both exogenous exposure and circulating blood mercury levels at the time the hair was formed [26]. Urinary total mercury primarily indicates inorganic mercury exposure and serves as the best biomarker for assessing elemental or inorganic mercury exposure, as it reflects mercury concentrations in the kidneys. Therefore, urine mercury levels are widely used in clinical screening procedures to estimate body burden and mercury toxicity. This urine biomarker is effective in assessing mercury exposure among individuals living near gold processing activities, including non-miners such as gold traders, children, and women, who are not directly involved in mining operations [26].
The study interprets and categorizes the results of laboratory measurements using reference standards from the German Human Biomonitoring (HBM) Commission and the World Health Organization (WHO) as presented in Table 2. Table 2 shows the classification matrix for those comparisons.
Table 2. Reference standards for T-Hg exposure
|
No. |
Critical Value |
Category |
|
1 |
Hair biomarker |
|
|
1.1 |
< 1 µg Hg/g hair |
Normal |
|
1.2 |
1 - < 5 µg Hg/g hair |
Alert |
|
1.3 |
$\geq$ 5 µg Hg/g hair |
High |
|
2 |
Urine biomarker |
|
|
2.1 |
< 7 µg/L urine (HBM1) |
Normal |
|
2.2 |
7 - < 25 µg/L Urin (HBM2) |
Alert |
|
2.3 |
$\geq$ 25 µg/L Urin (HBM2) |
High |
2.3.2 Health-related quality of life (HRQoL)
Data were collected through structured interviews using an EQ-5D-5L questionnaire, designed by EuroQol, to evaluate individual health status. This research assessed HRQoL using the pencil-and-paper EQ-5D-5L questionnaire version and the Visual Analogue Scale (VAS) instrument, as permitted by the EuroQol Group. The instruments have been validated and culturally adapted by Purba et al. [53], resulting in the reference value for the Indonesian EQ-5D-5L, to ensure conceptual equivalence and comprehension among local respondents. The enumerators, who were chosen from public health officers assisting in the interview process, helped translate each question and response in the EQ-5D-5L and VAS instruments into the local language, Sundanese, which is the respondents' native language in the study area.
The questionnaire consisted of two main sections. The first section is the Five Dimensions (5D) section, which assesses the respondent's condition based on five health-related dimensions, including mobility, self-care, daily activities, pain or discomfort, and anxiety or depression. Each dimension offered five response levels (5L) to indicate the severity of the problem experienced by the respondent, which included "no problems", "slight", "moderate", "severe", and "extreme". The second part is the VAS section, in which respondents rate their overall health on a visual scale ranging from 0 to 100, where 0 represents the worst health state and 100 represents the best health state. Respondents selected the level that best reflected their current health condition. The combination of the two assessments provided a comprehensive knowledge of the perceived health status, which is essential for evaluating the potential health effects of mercury exposure.
The variable of community health status was analyzed based on responses obtained from the questionnaire. The outputs from the five questions in both sections of the HRQoL questionnaire were converted into index scores using the Indonesian reference value set [53]. These converted values were then used to classify the overall health status of respondents into five categories: poor, somewhat poor, moderate, somewhat good, and good.
2.3.3 Socio-economic characteristics
The analysis of the relationship between socioeconomic factors and human mercury exposure was conducted separately for each respondent group using descriptive statistics. Statistical differences were tested using analysis of variance (ANOVA) at a confidence level of 0.05. To examine differences in total mercury (T-Hg) levels across groups based on qualitative variables such as education level, the Mann-Whitney U test was employed.
The Spearman correlation test was used to calculate correlations between mercury exposure values and quantitative socioeconomic variables, including age, length of residence, distance from residence to processing sites, number of household members, monthly income, and HRQoL scores. For categorical variables (both nominal and ordinal), the analysis applied Eta correlation, supported by comparative tests such as Mann-Whitney or Kruskal-Wallis.
3.1 Level of mercury contamination
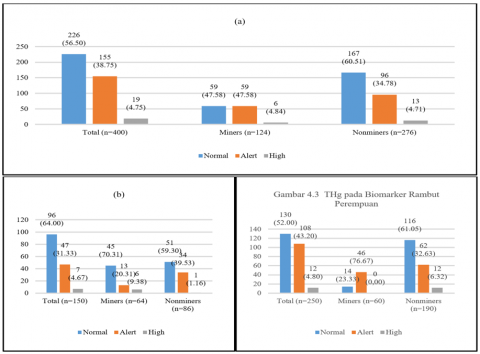
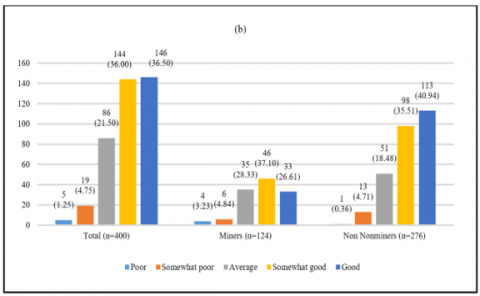
The average concentration of total mercury in respondents’ hair samples was 1.67 µg/g (n = 400), which falls within the “alert” category, although the majority (56.50%) remained in the normal range (Figure 2 (a)). When analyzed by gender, most male respondents (n = 150) exhibited mercury levels in hair within the normal category, including both those involved in ASGM (n = 64) and non-miners (n = 86), with more than 64% falling in the normal range as shown in Figure 2 (b).
Figure 2. T-Hg in hair biomarker of all respondents (a), men (b), and women (c)
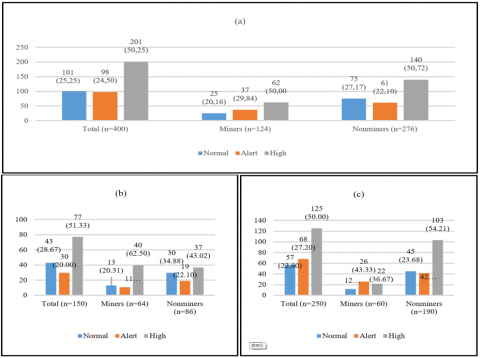
Figure 3. T-Hg in urine biomarker of all respondents (a), men (b), and women (c)
In contrast, among female respondents involved in ASGM (n = 60), the majority (76.67%) were in the alert category. However, among female non-ASGM respondents (n = 190), a larger proportion (61.05%) were still within the normal category (Figure 2 (c)). Overall, the percentage of female respondents exposed to mercury at alert and high levels (48%) was higher than that of male respondents (36.10%).
The average total mercury concentration in urine samples among all respondents was 35.81 µg/L, with levels of 31.71 µg/L for miners and 37.65 µg/L for non-miners. According to the German Human Biomonitoring (HBM) standards, these values fall within the high category as presented in Figure 3 (a).
Distribution analysis showed that the majority of respondents had mercury levels categorized as either alert or high, regardless of their involvement in ASGM. Notably, the percentage of respondents in the high category exceeded 50% in both groups. A similar pattern emerged across gender lines, where more than half of both male and female respondents, whether involved in ASGM or not, showed total urinary mercury concentrations at alert or high levels (Figures 3 (b) and (c)).
A comparative test was conducted to determine whether there is a significant difference in hair T-Hg and urine T-Hg levels between miners and non-miners. If a difference exists, the test also identifies which group has higher or lower levels of the variable. The following Table 3 is a summary of the Mann-Whitney comparison test results for hair and urine T-Hg data between miners and non-miners.
The summary results in Table 3 show that the p-values for hair and urine T-Hg levels in both groups are greater than 0.05, specifically 0.163 and 0.845, respectively. These values indicate that there is no significant difference in hair and urine T-Hg levels between miners and non-miners. These results suggest that the entire population living in the study area is facing the same risk level of mercury exposure, both through the consumption pathway, as indicated by T-Hg in hair samples, and the exposure pathway, as revealed by T-Hg in urine samples.
The results of total mercury testing in hair and urine biomarkers of all respondents revealed differences in risk levels as indicated by the two biomarkers. Mercury exposure levels in hair biomarkers for the majority of respondents remained within normal limits according to WHO standards. However, 43.50% of respondents fell into the alert to high exposure categories. In contrast, for urine biomarkers, 74.75% of respondents already fell into the alert and high categories according to German HBM reference values.
The presence of mercury in hair indicates exposure through air or the consumption of food and drinking water, suggesting that mercury risk affects not only miners but the entire community. This condition is supported by findings from other studies in the same or neighboring sub-districts, which have shown that soil and biota are already heavily contaminated [18, 21].
Although mercury exposure levels in this study location did not align with the previous study, that found hair mercury levels predominantly high, as found in other sub-districts in Sukabumi [7], South Sulawesi [14, 60], and Southeast Sulawesi [61], or in countries like Peru [62], the long-term risk remains significant. It is because, theoretically, mercury in hair is cumulative and persistent [63, 64].
Table 3. The comparison of hair and urine T-Hg levels
|
No |
Variable |
Miners |
Non-Miners |
P |
|
1 |
Hair T-Hg (µg/g) |
|
|
|
|
1.1 |
Mean ± SD |
1.33±1.77 |
1.82±8.18 |
0.163 |
|
1.2 |
Median |
1.03 |
0.83 |
|
|
1.3 |
Min-Max |
0.00-0.30 |
0.00-112.00 |
|
|
2 |
Urine T-Hg (µg/L) |
|
|
|
|
2.1 |
Mean ± SD |
31.71±31.65 |
37.65±44.68 |
0.845 |
|
2.2 |
Median |
1.03 |
0.83 |
|
|
2.3 |
Min-Max |
0.00-0.30 |
0.00-112.00 |
|
Urine mercury exposure levels in 74.75% of respondents already fall into the alert category (HBM I-HBM II) or even above HBM II thresholds [58]. The likely exposure pathways for urine biomarkers include direct contact or environmental exposure via air, water, or soil. According to observations and interviews, ore processing activities were carried out around the home, with some tromol (rotating drums) installed inside houses, and waste containing potential mercury was discharged nearby. Another critical exposure route is amalgam burning, which is also conducted within residential areas.
This study confirms the view of other researchers that urine is an appropriate biomarker for assessing acute mercury exposure through direct contact [64]. The high proportion of individuals whose urinary mercury levels exceeded HBM I and HBM II thresholds suggests that contamination occurs via both occupational and environmental routes [65], represented in this study by both miners and non-miners. These findings align with ASGM research in Mexico [66] but differ from studies in Ghana [26] and Ecuador [50], which reported that mercury exposure in urine among their respondents was generally below reference values.
Statistical testing showed no significant difference in mercury exposure levels in hair and urine between groups. This result contrasts with several other studies [67, 68] that found significantly higher exposure levels among miners compared to non-miners. Several factors may contribute, including the use of mercury for gold ore processing near residential areas, untreated mining waste discharge contaminating soil, water, and biota, and amalgam burning conducted in settlements. Combination of these factors create exposure risks for both miners and non-miners.
Residents in the study area primarily obtain staple foods and vegetables locally, either by growing them or purchasing them from local markets or vendors. Similarly, protein sources are usually purchased from local markets. However, previous research [18] has reported that food crops such as rice, cassava, and papaya grown in Waluran and Lengkong sub-districts are highly contaminated with mercury, exceeding the Indonesian National Agency of Drug and Food Control (BPOM) recommended limit of 0.03 ppm.
These findings also demonstrate that soil and wastewater media around ASGM processing facilities in the sampled sub-districts are heavily polluted, with values exceeding national standards for soil mercury pollution (Government Regulation No. 101 of 2014) and wastewater (Ministerial Regulation No. 202 of 2004) [69].
In terms of clean water sources, the majority of respondents (78.50%, n = 400) relied on wells, while 15.50% used rivers and springs, and 9.75% consumed bottled water. If well or spring water is contaminated with mercury, the persistent nature of this heavy metal in the environment means that exposure risks increase. This has been observed in studies conducted in Kenya [70], Togo [71] and Indonesia [72], where mercury contamination in well water may contribute up to 20-30% of weekly mercury intake [70].
A recent study in Simpenan Subdistrict [21], near the current study area, assessed environmental pollution in air, water, soil, sediments, biota, and crops from mercury use in ASGM. Ambient air mercury concentrations were found to be extremely high, ranging from 956-998ng/m³, indicating that amalgam burning continues in and around the research location. The study also concluded that mercury levels in soil, plants, and fish near ASGM operations were all within high contamination categories.
3.2 Health status of the community
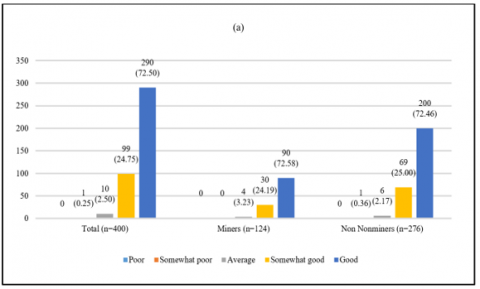
The HRQoL based on EQ-5D-5L assessment showed that the majority of respondents (over 72%), both miners and non-miners, reported good health status as presented in Figure 4 (a). Only 2.5% of the total respondents were categorized as having moderate health conditions, and less than 1% were in the somewhat poor health category. Similarly, in terms of VAS, most respondents rated their health as either good (36.5%) or somewhat good (36%). Only 4.75% of respondents rated their health as somewhat poor, and 1.25% as poor (Figure 4 (b)). However, at least 30 percent of all respondents reported experiencing slight to very severe problems in the health dimensions of mobility, self-care, daily activities, and bodily discomfort. Additionally, at least 20 percent of respondents reported experiencing slight problems in the dimension of depression or emotional disorders.
Specifically for the dimension of bodily discomfort, the proportion of respondents who reported experiencing slight to very severe problems was higher than that of those who reported no problems. The most common complaints included body aches, particularly in the legs, knees, lower back, or spine, as well as sensations of tingling, cramps, or numbness.
These findings contradict previous research [7] result, which found that various health problems were reported among residents with mercury exposure levels in the alert or high categories in other subdistricts of Sukabumi Regency. Theoretically, the German HBM developers also noted that health risks indicated by specific symptoms increase proportionally with rising critical mercury exposure levels in the body [58]. Other researchers have also linked ASGM activities with emerging health risks [73].
Figure 4. HRQoL based on EQ-5D-5L (a) and VAS (b)
Nevertheless, other studies have argued that HRQoL EQ-5D-5L scores do not always correlate directly with an individual’s actual health condition, and that the correlation between HRQoL EQ-5D-5L and VAS is not always linear. One study in Zimbabwe, for example, found that 42.5% of respondents reported excellent health despite having poor HRQoL scores [74]. While many symptoms may indicate mercury toxicity in the body, their association with HRQoL remains negative. One suspected contributing factor is education level; respondents with higher education tend to assess their health more accurately. Based on EQ-5D-5L assessment, the proportion of respondents in this study experiencing some to severe problems reached at least 20% in the dimension of depression or emotional disturbance. One known long-term effect of chronic mercury exposure, even at low levels, is fatigue, insomnia, or depression [75].
Additionally, based on observations and interviews, respondents' health complaints related to physical discomfort may also be associated with symptoms of mercury toxicity. Interviews with 400 respondents revealed various complaints and symptoms. The most commonly reported were muscle aches, numbness, tingling, cramps, gout, and joint pain (42%); stomach or gastrointestinal discomfort (15.25%); dizziness, headaches, and vertigo (11.75%); asthma, shortness of breath, and lung issues (8.25%); high cholesterol, hypertension, and high blood sugar (8.25%); liver, heart, and kidney disorders (2.75%); skin rashes or itching (2.75%); and vision problems (1%).
However, the health complaints or disorders experienced by respondents cannot be directly attributed to mercury exposure, as these complaints were self-reported and not supported by medical or laboratory tests, which is a methodological limitation of this study. To avoid subjective bias or overinterpretation of the association between individual discomfort and mercury exposure, future research should include clinical examinations or diagnostic testing to identify diseases or health disorders resulting from mercury exposure.
For comparison, several studies have linked health symptoms in communities with mercury exposure levels in the human body, including tremors, ataxia, vision loss, delayed reflexes, sensory nerve disorders, imbalance, headaches, muscle cramps, coughing, kidney dysfunction, hypertension, heart problems, stomach and intestinal issues, lung and respiratory disorders, tuberculosis, and skin diseases [14, 27, 46, 76-81].
Other researchers have even calculated that the global health risk attributable to mercury emissions from ASGM is equivalent to USD 7.1 million, or approximately 48.3% of the total revenue generated from ASGM gold production [37]. One recommended approach to improve health conditions and reduce ASGM-related risks is to increase education and training, particularly for artisanal miners [82].
3.3 Socio-economic characteristics and correlations with mercury contamination in humans
One of the objectives of this study is to analyze the correlation between socio-economic factors and human mercury exposure. The socio-economic factors include monthly income level, age, length of residence, gender, number of family members, distance from home to the gold processing site, and wealth, which comprises sub-variables such as home ownership and housing type.
The data on socio-economic characteristics are presented in Table A1. The majority of respondents reported a monthly income of up to IDR 1,500,000, both overall (n = 400), among miners (n = 124), and among non-miners (n = 276). The proportion of respondents with high or very high income levels is relatively balanced between mining and non-mining groups.
In terms of age, all respondents range from 15 to 90 years old. Age was grouped into 10-year intervals, with the highest proportions found in the 35-44 and 45-54 age groups, for both miners and non-miners. The residence duration variable shows a more even distribution, with the most common duration being 35-44 years for both groups.
Job opportunities in ASGM are relatively accessible to both men and women in Sukabumi Regency. However, excavation work is typically a male-dominated domain, while women generally participate in processing activities, such as ore pounding. In this study, the proportion of male respondents (37.50%) was lower than that of female respondents (62.50%). A total of 124 respondents (31%) were currently or previously involved in ASGM. However, among them, the number of male respondents (n = 64) involved in ASGM was slightly higher than the number of female respondents (n = 60).
The following variable is the number of family members. This study categorizes families into three groups: small families (maximum of 4 members), medium families (5 to 7 members), and large families (more than 7 members). The findings from the study site indicate that the proportion of small families is higher than the other two categories, both among mining and non-mining respondents.
The facilities for processing mining materials (locally known as gelundung or tromol) can be located inside or in the yard of a residence, meaning that the shortest possible distance from a house to a processing site is 0 meters. The majority of respondents, both miners and non-miners, fall under the "close distance" category (within 5km). Among the mining respondents, all were located within this close range. However, there are also processing sites situated at greater distances, over 10km away, particularly in Waluran Subdistrict.
The following variable is the level of household wealth, which in this study is indicated by home ownership status and housing type. Home ownership is classified into: privately owned, owned by parents (borrowed use), and official (government- or company provided) housing. The majority of respondents live in privately owned homes, followed by those living in borrowed homes from their parents or relatives and official residences. In terms of housing type, at least 50% of respondents live in permanent houses. The rest reside in semi-permanent or non-permanent houses, the latter typically being wooden stilt houses.
The correlation analysis began with a Kolmogorov–Smirnov normality test at a 95% confidence level for mercury exposure data and the socio-economic variables with numerical values (age, length of residence, distance to processing site, number of family members, monthly income, HRQoL, and VAS). The test results indicated that most data were not normally distributed. Therefore, correlation tests were conducted using the non-parametric Spearman's rank correlation test. A summary of the correlation test results between the numerical variables and T-Hg in hair and T-Hg in urine, based on the output from IBM SPSS for Windows version 26.0, at a 95% confidence level and p < 0.05, is presented in Table 4.
Table 4. Results of the Spearman's rank correlation test between the numerical variables and T-Hg in individuals
|
No. |
Variable |
Hair T-Hg |
Urine T-Hg |
|
1 |
Age (years) |
-0.057 |
-0.042 |
|
2 |
Residence duration (years) |
-0.057 |
0.011 |
|
3 |
Number of family members |
0.055 |
-0.006 |
|
4 |
Distance between house and processing facilities (m) |
0.036 |
-0.010 |
|
5 |
Monthly income (million IDR) |
0.180* |
-0.064 |
|
6 |
EQ-5D-5L |
-0.020 |
-0.050 |
|
7 |
VAS |
0.021 |
-0.041 |
The Spearman's rank correlation analysis between mercury exposure levels (T-Hg) in hair and urine and all numerical socio-economic variables including age, length of residence, number of family members, distance from residence to processing site, monthly income, EQ-5D-5L, and VAS showed that only one variable, it is monthly income, had a statistically significant correlation with T-Hg levels in hair (p < 0.05) (Table 4). The correlation coefficient was positive, indicating that individuals with higher monthly income tended to have higher mercury exposure levels in hair. An explanation is provided by previous research, which found that the desire to increase income is a strong motivator for engaging in ASGM activities, especially given the low income potential from alternative livelihoods [83].
However, the coefficient correlation (r = 0.180) indicates a weak linear relationship between respondents' monthly income and mercury exposure levels in their hair. In other words, an individual's monthly income level is not a strong predictor of their mercury exposure level. Other factors may contribute a more significant role in explaining mercury exposure levels. The cross-sectional nature of the study may also contribute to the weakness of this correlation. Therefore, this finding should be regarded as indicative rather than confirmatory evidence of exposure–cause relationship.
Meanwhile, for mercury exposure in urine, none of the socio-economic variables showed a statistically significant correlation. It implies that the level of individual mercury exposure is not correlated with age, length of residence, distance from residence to processing site, number of family members, monthly income level, EQ-5D-5L, or VAS scores.
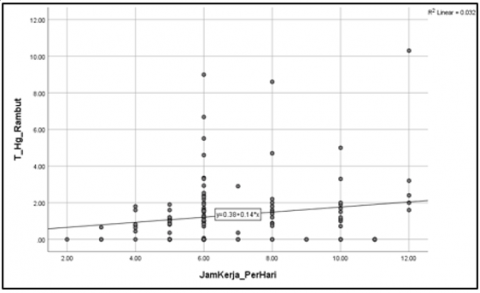
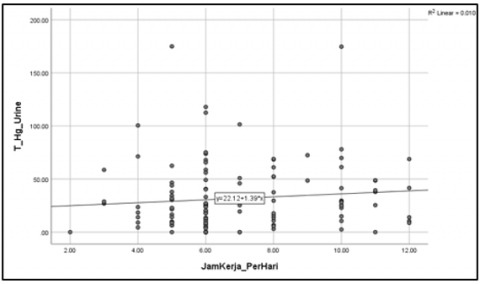
Specifically for miners, the analysis revealed a positive and statistically significant correlation between working hours and T-Hg levels in both hair and urine, with correlation coefficients of 0.179 and 0.131, respectively. It indicates that the longer an individual works, the higher the concentration of T-Hg in hair and urine, and vice versa as presented in Figures 5 (a) and (b).
However, the regression lines between working hours and total mercury (T-Hg) concentrations in hair and urine samples shown in Figure 5 appeared nearly flat, indicating a weak relationship. The findings imply that daily working duration alone is unlikely to be the primary factor determining mercury accumulation in the body. Other factors, such as differences in individual exposure intensity or irregular use of protective equipment, may also contribute to the level of mercury exposure. Furthermore, the multiple routes of exposure pathways in ASGM activities, including inhalation of mercury vapor during amalgamation, dermal contact, and indirect exposure through contaminated soil or food, may co-occur.
(a)
(b)
Figure 5. Correlation between working hours and T-Hg in hairs (a) dan urine (b)
The correlation between variables with categorical scales (both nominal and ordinal) was assessed using the Eta correlation test, supported by Mann-Whitney or Kruskal-Wallis comparison tests. Table A2 is a summary of the test results for the correlation between categorical variables, including gender, education level, house ownership, and housing type and T-Hg concentrations in hair and urine.
The correlation test results indicated that none of the categorical variables showed a statistically significant correlation with T-Hg levels in hair and urine, as reflected by the low Eta correlation coefficients. However, T-Hg levels in hair were significantly higher among female respondents compared to males (p < 0.05). The location of gold processing activities that are often situated within residential areas, sometimes even attached to the side or rear of houses, exposes women involved in processing activities such as crushing or grinding ore to prolonged exposure to processing dust [84] as well as potential mercury-containing waste. Furthermore, women who are not directly involved in mining or processing may still face elevated exposure risks, particularly through inhalation pathways, since the ambient air surrounding ASGM processing areas has been shown to contain high levels of mercury [21]. In addition, housing type also showed a statistically significant difference in relation to hair T-Hg levels. Respondents with the lowest level of wealth, as reflected by their housing type, had higher total mercury concentrations in their hair.
The correlation patterns between socio-economic variables and mercury exposure levels observed in this study are consistent with findings from other research. A study in Ghana reported that total mercury levels in individuals were not correlated with age, gender, or duration of exposure, but were positively correlated with length of residence in the area [26]. In contrast to the present study, other researchers found significant differences in urinary total mercury levels between miners and non-miners in ASGM areas in Ghana [85].
Meanwhile, research conducted in Colombia revealed that mercury exposure levels in hair and urine were not correlated, which was attributed to different exposure pathways reflected by each biomarker. Urinary mercury levels are associated with inhalation of mercury vapor during amalgamation processes in ASGM, whereas mercury in hair may result from dietary intake [86].
Several researchers have suggested that mercury contamination is more significantly correlated with knowledge levels, where low awareness contributes to higher exposure risks [54, 55]. Moreover, occupational choices are influenced by factors such as age, household size, education level, and the availability of alternative livelihoods [87]. In summary, findings from these studies suggest that mercury exposure levels are not always directly correlated with socio-economic variables, consistent with the results of this research. To adhere to the limitations of the correlation test between mercury exposure levels in individuals and socio economic factors, future studies could apply multivariable regression for better adjustment of confounding factors.
The high risk of mercury exposure among residents living near ASGM sites in Sukabumi provides important input for Indonesia's mercury reduction and elimination policies, as outlined in the NAP under the implementation of Presidential Regulation No. 21 of 2019. The detection of mercury exposure levels ranging from alert to high in hair samples (43.5% of total respondents) and urine samples (74.75% of total respondents), combined with the absence of significant statistical differences between genders or livelihood (miners and non-miners), suggests that mercury exposure risk from ASGM activities and multiple exposure pathways potentially affects the entire population.
The health assessment results also indicate that the government should establish biomonitoring programs for populations at risk, identified in this study as the entire community, as encouraged in Annex C of the Minamata Convention. The government can use these findings as a scientific and evidence-based reference for designing interventions aimed at achieving mercury reduction and elimination in the ASGM sector by 2025, in compliance with the ratification of the Minamata Convention.
This study identified varying levels of mercury exposure among individuals living near ASGM activities in the sub-districts of Ciemas, Waluran, and Lengkong, Sukabumi Regency, based on assessments using hair and urine biomarkers. The average total mercury concentration in hair was 1.67 µg/g (n = 400), which falls under the "alert" category according to WHO standards. A total of 43.50% of all respondents had hair mercury concentrations categorized as alert or high. In comparison, urinary total mercury concentrations were found to be higher, with an average of 35.81 µg/L, classified as high according to Germany's Human Biomonitoring (HBM) standards.
Statistical tests indicated no significant difference in total mercury levels between hair and urine biomarkers across miners and non-miners, suggesting that the entire population, regardless of involvement in ASGM, faces similar mercury exposure risks. These risks likely stem from direct contact, inhalation, or contaminated food and water sourced from areas surrounding ASGM operations, where environmental media such as air, soil, and biota (e.g., fish and crops), have already been contaminated with mercury.
Nevertheless, health assessments using the HRQoL instrument showed that the majority of respondents still perceived their health as good, despite reports of physical and emotional health issues from a portion of the population. Interviews revealed community complaints related to neurological, muscular, internal organ, high blood pressure, and respiratory problems.
Correlation analysis between socio-economic characteristics and mercury exposure levels indicated that only monthly income and work duration had a significant correlation with total mercury levels. This finding suggests that longer work duration, which increases contact with mercury during ore processing and amalgam burning, and is often driven by the motivation to increase income, is associated with higher mercury exposure risk.
Overall, in contrast to several previous studies, this research found that all populations living near ASGM face a similar risk of mercury exposure, regardless of their status as miners or non-miners, or male or female. This highlights the urgent need for intensive public awareness campaigns on the dangers of mercury to health and the environment, as well as strict control of its use in ASGM. Further research is needed to explore the link between reported health symptoms and mercury exposure, which can inform policy actions for mercury use control and community health interventions.
The authors would like to express their gratitude to the healthcare workers, village and sub-district government officials in Ciemas, Lengkong, and Waluran, as well as the Sukabumi District Government, for their valuable assistance in collecting hair and urine samples, as well as socio-economic data during the research.
Table A1. Socio-economic characteristics of the respondents
|
No. |
Variable and Criteria |
Frequency |
||
|
All (N = 400) |
Miners (n = 124) |
Non-Miners (n = 276) |
||
|
1 |
Monthly income (X = IDR…) |
|||
|
1.1 |
Low (X ≤ 1,500,000) |
173 (43.25) |
65 (52.42) |
108 (39.13) |
|
1.2 |
Moderate (1,500m000 < X ≤ 2,500,000) |
99 (24.75) |
35 (28.23) |
64 (23.19) |
|
1.3 |
High (2,500,000 < X ≤ 3,500,000) |
65 (16.25) |
12 (9.68) |
53 (19.20) |
|
1.4 |
Very high (X > 3,500,000) |
63 (15.75) |
12 (9.68) |
51 (18.48) |
|
2 |
Age (years) |
|||
|
2.1 |
15-24 |
27 (6.75) |
8 (6.45) |
19 (6.88) |
|
2.2 |
25-34 |
60 (15.00) |
17 (13.71) |
43 (15.58) |
|
2.3 |
35-44 |
101 (25.25) |
36 (29.03) |
65 (23.55) |
|
2.4 |
45-54 |
102 (25.50) |
36 (29.03) |
65 (23.55) |
|
2.5 |
55-64 |
74 (18.50) |
15 (12.10) |
59 (21.38) |
|
2.6 |
65+ |
36 (9.00) |
12 (9.68) |
24 (8.70) |
|
3 |
Residence duration (years) |
|||
|
3.1 |
0-14 |
47 (11.75) |
11 (8.87) |
36 (13.04) |
|
3.2 |
15-24 |
51 (12.75) |
14 (11.29) |
37 (13.41) |
|
3.3 |
25-34 |
58 (14.50) |
17 (13.71) |
41 (14.86) |
|
3.4 |
35-44 |
80 (20.00) |
28 (22.58) |
52 (18.84) |
|
3.5 |
45-54 |
77 (19.25) |
29 (23.39) |
48 (17.39) |
|
3.6 |
55-64 |
57 (14.25) |
13 (10.48) |
44 (15.94) |
|
3.7 |
65+ |
30 (7.50) |
12 (9.68) |
18 (6.52) |
|
4 |
Gender |
|
|
|
|
4.1 |
Men |
150 (37.50) |
64 (42.67) |
86 (57.33) |
|
4.2 |
Women |
250 (62.50) |
60 (24.00) |
190 (76.00) |
|
5 |
Number of family members (X = …people) |
|||
|
5.1 |
Small (0 < X ≤4) |
315 (78.75) |
105 (84.68) |
210 (76.09) |
|
5.2 |
Medium (4 < X ≤7) |
82 (20.50) |
18 (14.52) |
64 (23.19) |
|
5.3 |
Large (X > 7) |
3 (0.75) |
1 (0.81) |
2 (0.72) |
|
6 |
Distance between house and mining processing site (X = ….km) |
|||
|
6.1 |
Near (0 < X ≤ 5) |
361 (90.25) |
124 (100.00) |
239 (86.59) |
|
6.2 |
Medium (5 < X≤ 10) |
7 (1.75) |
0 (0.00) |
6 (2.17) |
|
6.3 |
Far (X > 10) |
32 (8.00) |
0 (0.00) |
31 (11.23) |
|
7 |
House ownership |
|||
|
7.1 |
Private |
360 (90.00) |
122 (98.39) |
238 (86.23) |
|
7.2 |
Parents or relatives |
24 (6.00) |
1 (0.81) |
23 (8.33) |
|
7.3 |
Employee housing |
16 (4.00) |
1 (0.81) |
15 (5.43) |
|
8 |
Housing type |
|
|
|
|
8.1 |
Permanent |
274 (68.50) |
69 (55.64) |
205 (74.27) |
|
8.2 |
Semi-permanent |
115 (28.75) |
54 (43.55) |
61 (22.10) |
|
8.3 |
Non-permanent |
11 (4.00) |
1 (0.81) |
10 (3.62) |
Table A2. Results of correlation test between categorical variables and T-Hg
|
No. |
Variable |
T-Hg in Hair |
T-Hg in Urine |
||||||
|
Mean |
SD |
Eta corr |
p |
Mean |
SD |
Eta corr |
p |
||
|
1 |
Gender |
|
|
|
|
|
|
|
|
|
1.1 |
Men |
1.00 |
1.74 |
0.075 |
0.000** |
32.52 |
35.54 |
0.062 |
0.310 |
|
1.3 |
Women |
2.07 |
8.57 |
|
|
37.78 |
44.10 |
|
|
|
2 |
Education |
|
|
|
|
|
|
|
|
|
2.1 |
None |
4.31 |
6.10 |
0.143 |
0.927 |
23.28 |
32.92 |
0.048 |
0.387 |
|
2.2 |
Primary School |
1.07 |
1.39 |
|
|
34.80 |
43.11 |
|
|
|
2.3 |
Junior High School |
3.58 |
14.71 |
|
|
37.40 |
34.03 |
|
|
|
2.4 |
Senior High School |
2.52 |
9.30 |
|
|
36.34 |
42.22 |
|
|
|
2.5 |
Higher Education |
0.84 |
0.66 |
|
|
41.27 |
36.14 |
|
|
|
3 |
House ownership |
|
|
|
|
|
|
|
|
|
3.1 |
Employee housing |
0.91 |
0.29 |
0.098 |
0.277 |
54.12 |
60.25 |
0.091 |
0.472 |
|
3.2 |
Parents or relative |
4.28 |
14.50 |
|
|
36.52 |
41.07 |
|
|
|
3.3 |
Private |
1.53 |
6.20 |
|
|
34.95 |
40.06 |
|
|
|
4 |
Housing type |
|
|
|
|
|
|
|
|
|
4.1 |
Non-permanent |
7.61 |
21.39 |
0.153 |
0.026* |
26.92 |
22.58 |
0.04 |
0.951 |
|
4.2 |
Semi-permanent |
0.99 |
1.58 |
|
|
35.01 |
38.04 |
|
|
|
4.3 |
Permanent |
1.72 |
7.04 |
|
|
36.50 |
42.97 |
|
|
[1] Peluso, N.L. (2018). Entangled territories in small-scale gold mining frontiers: Labor practices, property, and secrets in Indonesian gold country. World Development, 101: 400-416. https://doi.org/10.1016/j.worlddev.2016.11.003
[2] Ismawati, Y. (2011). Opening the Pandora’s box of poboya: The social and environmental production of suffering in central Sulawesi, Indonesia. Master's Thesis, Oxford University, Oxford, UK.
[3] Meutia, A.A., Lumowa, R., Sakakibara, M. (2022). Indonesian artisanal and small-scale gold mining-A narrative literature review. International Journal of Environmental Research and Public Health, 19(7): 3955. https://doi.org/10.3390/ijerph19073955
[4] Bansah, K.J., Dumakor-Dupey, N.K., Kansake, B.A., Assan, E., Bekui, P. (2018). Socioeconomic and environmental assessment of informal artisanal and small-scale mining in Ghana. Journal of Cleaner Production, 202: 465-475. https://doi.org/10.1016/j.jclepro.2018.08.150
[5] Prabawa, F.Y., Zagloel, T.Y., Koestoer, R.H., Abdini, C. (2019). Improving the economy of community's gold mining sector in Indonesia with the usage of efficient and clean technology in gold extracting process. Advances in Environmental Sciences, 11(3): 195-207.
[6] Basri, B., Sakakibara, M., Ratnawati, R. (2017). Economic features of the artisanal and small-scale gold mining industry in Bombana, Southeast Sulawesi, Indonesia. IOP Conference Series: Earth and Environmental Science, 71(1): 012016. https://doi.org/10.1088/1755-1315/71/1/012016
[7] Harianja, A.H., Saragih, G.S., Fauzi, R., Hidayat, M.Y., Syofyan, Y., Tapriziah, E.R., Kartiningsih, S.E. (2020). Mercury exposure in artisanal and small-scale gold mining communities in Sukabumi, Indonesia. Journal of Health and Pollution, 10(28): 201209. https://doi.org/10.5696/2156-9614-10.28.201209
[8] Komatsu, S., Tanaka, K., Sakakibara, M., Arifin, Y.I., Pateda, S.M., Manyoe, I.N. (2020). Sociodemographic attributes and dependency on artisanal and small-scale gold mining: The case of rural Gorontalo, Indonesia. IOP Conference Series: Earth and Environmental Science, 589(1): 012020. https://doi.org/10.1088/1755-1315/589/1/012020
[9] Ahenkan, A., Suleiman, N., Boon, E.K. (2020). Small-scale mining and sustainable rurality in the Atiwa district of Ghana. Journal of Rural and Community Development, 15(4): 58-80.
[10] Balzino, M., Seccatore, J., Marin, T., De Tomi, G., Veiga, M.M. (2015). Gold losses and mercury recovery in artisanal gold mining on the Madeira River, Brazil. Journal of Cleaner Production, 102: 370-377. https://doi.org/10.1016/j.jclepro.2015.05.012
[11] Hilson, G. (2010). ‘Once a miner, always a miner’: Poverty and livelihood diversification in Akwatia, Ghana. Journal of Rural Studies, 26(3): 296-307. https://doi.org/10.1016/j.jrurstud.2010.01.002
[12] Palapa, T.M., Maramis, A.A. (2015). Pollution status and mercury sedimentation in small river near amalgamation and cyanidation units of Talawaan-Tatelu gold mining, North Sulawesi. Journal of Degraded and Mining Lands Management, 2(3): 335-340. https://doi.org/10.15243/jdmlm.2015.023.335
[13] Andri, D.H., Anies, A., Suharyo, H. (2011). Kadar merkuri pada rambut masyarakat di sekitar penambangan emas tanpa ijin. Media Medika Indonesiana, 45(3): 181-187.
[14] Abbas, H.H., Sakakibara, M., Sera, K., Arma, L.H. (2017). Mercury exposure and health problems in urban artisanal gold mining (UAGM) in Makassar, South Sulawesi, Indonesia. Geosciences, 7(3): 44. https://doi.org/10.3390/geosciences7030044
[15] Gafur, N.A., Sakakibara, M., Sano, S., Sera, K. (2018). A case study of heavy metal pollution in water of Bone River by artisanal small-scale gold mine activities in eastern part of Gorontalo, Indonesia. Water, 10(11): 1507. https://doi.org/10.3390/w10111507
[16] Basri, Sakakibara, M., Sera, K. (2020). Mercury in soil and forage plants from artisanal and small-scale gold mining in the Bombana area, Indonesia. Toxics, 8(1): 15. https://doi.org/10.3390/toxics8010015
[17] Baiq, D.K. (2018). ASGM status in West Nusa Tenggara Province, Indonesia. Journal of Degraded and Mining Lands Management, 5(2): 1077-1084. https://doi.org/10.15243/jdmlm.2018.052.1077
[18] Saragih, G.S., Tapriziah, E.R., Syofyan, Y., Masitoh, S., Pandiangan, Y.S.H., Andriantoro, A. (2021). Mercury contamination in selected edible plants and soil from artisanal and small-scale gold mining in Sukabumi Regency, Indonesia. Makara Journal of Science, 25(4): 222-228. https://doi.org/10.7454/mss.v25i4.1280
[19] Basri, Sakakibara, M., Sera, K. (2017). Current mercury exposure from artisanal and small-scale gold mining in Bombana, Southeast Sulawesi, Indonesia-Future Significant Health Risks. Toxics, 5(1): 7. https://doi.org/10.3390/toxics5010007
[20] Junaidi, M., Krisnayanti, B.D., Juharfa, Anderson, C. (2019). Risk of mercury exposure from fish consumption at artisanal small-scale gold mining areas in West Nusa Tenggara, Indonesia. Journal of Health and Pollution, 9(21): 190302. https://doi.org/10.5696/2156-9614-9.21.190302
[21] Nuryanty, C.D., Riani, E., Abidin, Z., Sutjahjo, S.H., Riyadi, A. (2024). Mercury contamination from artisanal small-scale gold mining activities in Simpenan District, Sukabumi Regency, West Java, Indonesia. Asian Journal of Water, Environment and Pollution, 21(4): 83-89. https://doi.org/10.3233/AJW240049
[22] Sumantri, A., Laelasari, E., Junita, N.R., Nasrudin, N. (2014). Logam merkuri pada pekerja penambangan emas tanpa izin. Kesmas, 8(8): 398-403. https://doi.org/10.21109/kesmas.v8i8.411
[23] Zaharani, F., Salami, I.R.S. (2015). Kandungan merkuri pada urin dan rambut sebagai indikasi paparan merkuri terhadap pekerja tambang emas tanpa izin (Peti) di desa pasar terusan kecamatan muara bulian kabupaten batanghari-jambi. Journal of Environmental Engineering ITB, 21(2): 169-179. https://doi.org/10.5614/jtl.2015.21.2.7
[24] Soprima, M., Kusnoputranto, H., Inswiasri, I. (2016). Community health risk assessment due to disposed mercury at artisanal gold mining in Lebak district, Banten. Jurnal Ekologi Kesehatan, 14(4): 296-308. https://doi.org/10.22435/jek.v14i4.4708.296-308
[25] Hagan, N., Robins, N., Hsu-Kim, H., Halabi, S., Espinoza Gonzales, R.D., Ecos, E., Richter, D., Vandenberg, J. (2015). Mercury hair levels and factors that influence exposure for residents of Huancavelica, Peru. Environmental Geochemistry and Health, 37(3): 507-514. https://doi.org/10.1007/s10653-014-9665-9
[26] Kwaansa-Ansah, E.E., Armah, E.K., Opoku, F. (2019). Assessment of total mercury in hair, urine and fingernails of small-scale gold miners in the Amanse West district, Ghana. Journal of Health and Pollution, 9(21): 190306. https://doi.org/10.5696/2156-9614-9.21.190306
[27] Sofia, S., Husodo, A.H., Sugiharto, E. (2016). Acute and chronic toxicity of mercury exposure in seafood and human populations near a small-scale gold mining area. International Journal of Public Health Science (IJPHS), 5(3): 257-266. https://doi.org/10.11591/ijphs.v5i3.4794
[28] Bernaudat, L., Keane, S. (2013). Partnership on reducing mercury in artisanal and small-scale gold mining (ASGM). E3S Web of Conferences, Vol. 1. https://doi.org/10.1051/e3sconf/20130136003
[29] Özyurt, Z., Türkoğlu, İ., Bahçeci, F. (2025). Investigation of biodiversity awareness and conservation behaviors on science teachers candidates. Challenges in Sustainability, 13(1): 97-109. https://doi.org/10.56578/cis130107
[30] Soemarwoto, R., Ellen, R. (2010). Gold mining and changing perceptions of risk in West Java. Human Organization, 69(3): 233-241. https://doi.org/10.17730/humo.69.3.gk887801m1476105
[31] Espejo, J.C., Messinger, M., Román-Dañobeytia, F., Ascorra, C., Fernandez, L.E., Silman, M. (2018). Deforestation and forest degradation due to gold mining in the Peruvian Amazon: A 34-year perspective. Remote Sensing, 10(12): 1903. https://doi.org/10.3390/rs10121903
[32] Mata, M., Hlaváček, P. (2025). Navigating sustainability in lithium extraction: Local perceptions of environmental and economic impacts in the Cínovec Region, Czech Republic. Challenges in Sustainability, 13(2): 254-265. https://doi.org/10.56578/cis130207
[33] Prescott, G.W., Baird, M., Geenen, S., Nkuba, B., Phelps, J., Webb, E.L. (2022). Formalizing artisanal and small-scale gold mining: A grand challenge of the Minamata Convention. One Earth, 5(3): 242-251. https://doi.org/10.1016/j.oneear.2022.02.005
[34] Cegan, J.C., Filion, A.M., Keisler, J.M., Linkov, I. (2017). Trends and applications of multi-criteria decision analysis in environmental sciences: Literature review. Environment Systems and Decisions, 37(2): 123-133. https://doi.org/10.1007/s10669-017-9642-9
[35] Hämäläinen, R.P. (2015). Behavioural issues in environmental modelling-the missing perspective. Environmental Modelling & Software, 73: 244-253. https://doi.org/10.1016/j.envsoft.2015.08.019
[36] Miller, G.T., Spoolman, S.E. (2016). Environmental Science (15th Edition). Cengage Learning, Boston, USA.
[37] Pang, Q., Gu, J., Wang, H., Zhang, Y. (2022). Global health impact of atmospheric mercury emissions from artisanal and small-scale gold mining. iScience, 25(9): 104881. https://doi.org/10.1016/j.isci.2022.104881
[38] Bank, M.S. (2020). The mercury science-policy interface: History, evolution and progress of the Minamata Convention. Science of the Total Environment, 722: 137832. https://doi.org/10.1016/j.scitotenv.2020.137832
[39] Adeola, F.O. (2020). Global impact of chemicals and toxic substances on human health and the environment. In Handbook of Global Health. Cham: Springer International Publishing, pp. 1-30. https://doi.org/10.1007/978-3-030-05325-3_96-1
[40] Cunningham, W.P., Cunningham, M.A. (2012). Environmental Science: A Global Concern (12th Edition). McGraw-Hill, New York.
[41] Dórea, J.G. (2021). Exposure to environmental neurotoxic substances and neurodevelopment in children from Latin America and the Caribbean. Environmental Research, 192: 110199. https://doi.org/10.1016/j.envres.2020.110199
[42] Kolbinger, V., Engström, K., Berger, U., Bose-O’Reilly, S. (2019). Polymorphisms in potential mercury transporter ABCC2 and neurotoxic symptoms in populations exposed to mercury vapor from goldmining. Environmental Research, 176: 108512. https://doi.org/10.1016/j.envres.2019.05.043
[43] Suhelmi, R., Amqam, H., Thaha, R.M., Mallongi, A., Daud, A., Ishaq, H. (2020). The relationship of mercury exposure with neurological problems in artisanal gold in Makassar city. Reviews on Environmental Health, 35(3): 265-269. https://doi.org/10.1515/reveh-2020-0034
[44] Hairat, U., Hartono, B. (2019). Analysis of peripheral neuropathy disorders in humans from mercury exposure: A systematic review. Indian Journal of Public Health Research & Development, 10(3): 476-481. https://doi.org/10.5958/0976-5506.2019.00542.4
[45] Coulibaly, G., Sanou, G., Sanon, M., Lengani, A.H., Bonzi, J.Y., Semde, A. (2020). Clinical, paraclinical, and evolutionary profiles of kidney failure in gold miners hospitalized in a nephrological service in a sub-Saharan African country. International Journal of Nephrology, 2020(1): 4282969. https://doi.org/10.1155/2020/4282969
[46] Pateda, S.M., Sakakibara, M., Sera, K. (2018). Lung function assessment as an early biomonitor of mercury-induced health disorders in artisanal and small-scale gold mining areas in Indonesia. International Journal of Environmental Research and Public Health, 15(11): 2480. https://doi.org/10.3390/ijerph15112480
[47] Rajaee, M., Yee, A.K., Long, R.N., Renne, E.P., Robins, T.G., Basu, N. (2017). Pulmonary function and respiratory health of rural farmers and artisanal and small scale gold miners in Ghana. Environmental Research, 158: 522-530. https://doi.org/10.1016/j.envres.2017.07.011
[48] Du, B., Li, P., Feng, X., Qiu, G., Zhou, J., Maurice, L. (2016). Mercury exposure in children of the Wanshan mercury mining area, Guizhou, China. International Journal of Environmental Research and Public Health, 13(11): 1107. https://doi.org/10.3390/ijerph13111107
[49] Pino, A., Bocca, B., Forte, G., Majorani, C., Petrucci, F., Senofonte, O., Alimonti, A. (2018). Determination of mercury in hair of children. Toxicology Letters, 298: 25-32. https://doi.org/10.1016/j.toxlet.2018.06.1215
[50] Schutzmeier, P., Berger, U., Bose-O’Reilly, S. (2017). Gold mining in Ecuador: A cross-sectional assessment of mercury in urine and medical symptoms in miners from Portovelo/Zaruma. International Journal of Environmental Research and Public Health, 14(1): 34. https://doi.org/10.3390/ijerph14010034
[51] Steckling, N., Tobollik, M., Plass, D., Hornberg, C., Ericson, B., Fuller, R., Bose-O’Reilly, S. (2017). Global burden of disease of mercury used in artisanal small-scale gold mining. Annals of Global Health, 83(2): 234-247. https://doi.org/10.1016/j.aogh.2016.12.005
[52] Becker, J., Bose-O’Reilly, S., Shoko, D., Singo, J., Steckling-Muschack, N. (2020). Comparing the self-reported health-related quality of life (HRQoL) of artisanal and small-scale gold miners and the urban population in Zimbabwe using the EuroQol (EQ-5D-3L+C) questionnaire: A cross-sectional study. Health and Quality of Life Outcomes, 18(1): 253. https://doi.org/10.1186/s12955-020-01475-0
[53] Purba, F.D., Hunfeld, J.A.M., Iskandarsyah, A., Fitriana, T.S., Sadarjoen, S.S., Ramos-Goñi, J.M., Passchier, J., Busschbach, J.J.V. (2017). The Indonesian EQ-5D-5L value set. PharmacoEconomics, 35(11): 1153-1165. https://doi.org/10.1007/s40273-017-0538-9
[54] Budnik, L.T., Casteleyn, L. (2019). Mercury pollution in modern times and its socio-medical consequences. Science of the Total Environment, 654: 720-734. https://doi.org/10.1016/j.scitotenv.2018.10.408
[55] Brugger, F., Zanetti, J. (2020). “In my village, everyone uses the tractor”: Gold mining, agriculture and social transformation in rural Burkina Faso. The Extractive Industries and Society, 7(3): 940-953. https://doi.org/10.1016/j.exis.2020.06.003
[56] Setiana, N., Syahnur, S. (2018). The impact of gold mining on the socio-economic and environmental life of the community in Beutong District, Nagan Raya Regency. Jurnal Ilmiah Mahasiswa Ekonomi Pembangunan, 3(4): 584-594. https://jim.usk.ac.id/EKP/article/view/10607.
[57] Suhartini, S., Abubakar, A. (2017). Socio economic impacts and policy of artisanal small-scale gold mining in relation to sustainable agriculture: A case study at Sekotong of West Lombok. Journal of Degraded and Mining Lands Management, 4(3): 789. https://doi.org/10.15243/jdmlm.2017.043.789
[58] Schulz, C., Angerer, J., Ewers, U., Kolossa-Gehring, M. (2007). The German human biomonitoring commission. International Journal of Hygiene and Environmental Health, 210(3-4): 373-382. https://doi.org/10.1016/j.ijheh.2007.01.035
[59] Arifin, Y.I., Sakakibara, M., Sera, K. (2015). Impacts of artisanal and small-scale gold mining (ASGM) on environment and human health of Gorontalo Utara Regency, Gorontalo Province, Indonesia. Geosciences, 5(2): 160-176. https://doi.org/10.3390/geosciences5020160
[60] Abbas, H.H., Sakakibara, M., Sera, K., Arma, L.H., Sididi, M. (2020). Socioeconomic and mercury exposure to the goldsmiths in Manggal subdistrict of urban artisanal gold mining (UAGM) area in Makassar, South Sulawesi, Indonesia. IOP Conference Series: Earth and Environmental Science, 589(1): 012015. https://doi.org/10.1088/1755-1315/589/1/012015
[61] Puluhulawa, F., Harun, A.A. (2019). Policy formalization of artisanal and small-scale gold mining (ASGM) post-ratification of Minamata Convention for sustainability (case study of ASGM Gorontalo). E3S Web of Conferences, 125: 02006. https://doi.org/10.1051/e3sconf/201912502006
[62] Feingold, B.J., Berky, A., Hsu-Kim, H., Jurado, E.R., Pan, W.K. (2020). Population-based dietary exposure to mercury through fish consumption in the Southern Peruvian Amazon. Environmental Research, 183: 108720. https://doi.org/10.1016/j.envres.2019.108720
[63] Queipo-Abad, S., González, P.R., Martínez-Morillo, E., Davis, W.C., Alonso, J.I.G. (2019). Concentration of mercury species in hair, blood and urine of individuals occupationally exposed to gaseous elemental mercury in Asturias (Spain) and its comparison with individuals from a control group formed by close relatives. Science of the Total Environment, 672: 314-323. https://doi.org/10.1016/j.scitotenv.2019.03.367
[64] Sinaga, H., Wahid, R.S.A., Raudah, S. (2023). Literature review: Gambaran efektivitas pemeriksaan keracunan merkuri dengan sampel biologis: Literature review: Description of the effevtiveness of mercury poisoning examination using biological sample. Borneo Journal of Medical Laboratory Technology, 6(1): 442-449. https://doi.org/10.33084/bjmlt.v6i1.6086
[65] Mambrey, V., Rakete, S., Tobollik, M., Shoko, D., Moyo, D., Schutzmeier, P., Steckling-Muschack, N., Muteti-Fana, S., Bose-O’Reilly, S. (2020). Artisanal and small-scale gold mining: A cross-sectional assessment of occupational mercury exposure and exposure risk factors in Kadoma and Shurugwi, Zimbabwe. Environmental Research, 184: 109379. https://doi.org/10.1016/j.envres.2020.109379
[66] Saldaña-Villanueva, K., Pérez-Vázquez, F.J., Ávila-García, I.P., Méndez-Rodríguez, K.B., Carrizalez-Yáñez, L., Gavilán-García, A., Vargas-Morales, J.M., Van-Brussel, E., Diaz-Barriga, F. (2022). A preliminary study on health impacts of Mexican mercury mining workers in a context of precarious employment. Journal of Trace Elements in Medicine and Biology, 71: 126925. https://doi.org/10.1016/j.jtemb.2022.126925
[67] Basu, N., Horvat, M., Evers, D.C., Zastenskaya, I., Weihe, P., Tempowski, J. (2018). A state-of-the-science review of mercury biomarkers in human populations worldwide between 2000 and 2018. Environmental Health Perspectives, 126(10): 106001. https://doi.org/10.1289/EHP3904
[68] Suárez-Criado, L., Rodríguez-González, P., Marrugo-Negrete, J., Alonso, J.I.G., Díez, S. (2023). Determination of methylmercury and inorganic mercury in human hair samples of individuals from Colombian gold mining regions by double spiking isotope dilution and GC-ICP-MS. Environmental Research, 231: 115970. https://doi.org/10.1016/j.envres.2023.115970
[69] Banunaek, Z.A. (2016). Pencemaran merkuri di lahan pertambangan emas rakyat dan strategi pengendaliannya. Masters thesis, Institut Teknologi Sepuluh Nopember Surabaya. https://repository.its.ac.id/72867/.
[70] King, D., Watts, M., Hamilton, E., Mortimer, R., Coffey, M., Osano, O., Di Bonito, M. (2024). Mercury speciation in environmental samples associated with artisanal small-scale gold mines using a novel solid-phase extraction approach to sample collection and preservation. Environmental Geochemistry and Health, 46(11): 481. https://doi.org/10.1007/s10653-024-02187-w
[71] Soumaoro, I., Pitala, W., Gnandi, K., Kokou, T. (2021). Health risk assessment of heavy metal accumulation in broiler chickens and heavy metal removal in drinking water using Moringa oleifera seeds in Lomé, Togo. Journal of Health and Pollution, 11(31): 210911. https://doi.org/10.5696/2156-9614-11.31.210911
[72] Johari, H.I., Rahmawati, D. (2020). Mercury contamination in groundwater from artisanal and small scale gold mining activities: A case study of southern Lombok coast, West Nusa Tenggara province. IOP Conference Series: Earth and Environmental Science, 413(1): 012016. https://doi.org/10.1088/1755-1315/413/1/012016
[73] Schreer, V. (2021). ‘Only gold can become hope’: Resource rushes and risky conviviality in Indonesian Borneo. Ethnos, 86(5): 920-942. https://doi.org/10.1080/00141844.2020.1743337
[74] Butscher, F.M., Rakete, S., Tobollik, M., Mambrey, V., Moyo, D., Shoko, D., Muteti-Fana, S., Steckling-Muschack, N., Bose-O’reilly, S. (2020). Health-related quality of life (EQ-5D+C) among people living in artisanal and small-scale gold mining areas in Zimbabwe: A cross-sectional study. Health and Quality of Life Outcomes, 18(1): 284. https://doi.org/10.1186/s12955-020-01530-w
[75] Abdelaal, A., Sultan, M., Abotalib, A.Z., Bedair, M., Krishnamurthy, R.V., Elhebiry, M. (2023). Emerging mercury and methylmercury contamination from new artisanal and small-scale gold mining along the Nile valley, Egypt. Environmental Science and Pollution Research, 30(18): 52514-52534. https://doi.org/10.1007/s11356-023-25895-9
[76] Bose-O’Reilly, S., Bernaudat, L., Siebert, U., Roider, G., Nowak, D., Drasch, G. (2017). Signs and symptoms of mercury-exposed gold miners. International Journal of Occupational Medicine and Environmental Health, 30(2): 249-269. https://doi.org/10.13075/ijomeh.1896.00715
[77] Ekawanti, A., Krisnayanti, B.D. (2015). Effect of mercury exposure on renal function and hematological parameters among artisanal and small-scale gold miners at Sekotong, West Lombok, Indonesia. Journal of Health and Pollution, 5(9): 25-32. https://doi.org/10.5696/2156-9614-5-9.25
[78] Entwistle, J.A., Hursthouse, A.S., Marinho Reis, P.A., Stewart, A.G. (2019). Metalliferous mine dust: Human health impacts and the potential determinants of disease in mining communities. Current Pollution Reports, 5(3): 67-83. https://doi.org/10.1007/s40726-019-00108-5
[79] Genchi, G., Sinicropi, M.S., Carocci, A., Lauria, G., Catalano, A. (2017). Mercury exposure and heart diseases. International Journal of Environmental Research and Public Health, 14(1): 74. https://doi.org/10.3390/ijerph14010074
[80] Stewart, A.G. (2020). Mining is bad for health: A voyage of discovery. Environmental Geochemistry and Health, 42(4): 1153-1165. https://doi.org/10.1007/s10653-019-00367-7
[81] Lopes-Araújo, A., Arrifano, G.P., Macchi, B.M., Augusto-Oliveira, M., Santos-Sacramento, L., Rodríguez Martín-Doimeadios, R.C., Jiménez-Moreno, M., Martins Filho, A.J., Alvarez-Leite, J.I., Oriá, R.B., do Nascimento, J.L.M., Crespo-Lopez, M.E. (2023). Hair mercury is associated with dyslipidemia and cardiovascular risk: An anthropometric, biochemical and genetic cross-sectional study of Amazonian vulnerable populations. Environmental Research, 229: 115971. https://doi.org/10.1016/j.envres.2023.115971
[82] Becker, J., Furu, P., Singo, J., Shoko, D., Elbel, J., Bose-O’Reilly, S., Steckling-Muschack, N. (2021). Determinants of health and health needs assessment of artisanal and small-scale gold miners in Kadoma, Zimbabwe: A mixed method approach. Environmental Research, 197: 111081. https://doi.org/10.1016/j.envres.2021.111081
[83] Astuti, W.F., Agusta, I., Siwi, M. (2017). Dampak aktivitas pertambangan emas tanpa izin terhadap kesejahteraan rumah tangga gurandil. Jurnal Sains Komunikasi dan Pengembangan Masyarakat [JSKPM], 1(3): 317-338. https://doi.org/10.29244/jskpm.1.3.317-338
[84] Adomako, J., Hausermann, H. (2023). Gendered mining landscapes and health implications in Ghana's artisanal and small-scale gold mining industry. Journal of Rural Studies, 97: 385-394. https://doi.org/10.1016/j.jrurstud.2022.12.028
[85] Ovadje, L., Calys-Tagoe, B.N., Clarke, E., Basu, N. (2021). Registration status, mercury exposure biomarkers, and neuropsychological assessment of artisanal and small-scale gold miners (ASGM) from the western region of Ghana. Environmental Research, 201: 111639. https://doi.org/10.1016/j.envres.2021.111639
[86] Calao-Ramos, C., Bravo, A.G., Paternina-Uribe, R., Marrugo-Negrete, J., Díez, S. (2021). Occupational human exposure to mercury in artisanal small-scale gold mining communities of Colombia. Environment International, 146: 106216. https://doi.org/10.1016/j.envint.2020.106216
[87] Ibrahim, I., Baiquni, M., Ritohardoyo, S., Setiadi, S. (2016). Characteristics of poverty in rural communities of gold mining district area west Sumbawa. MIMBAR: Jurnal Sosial dan Pembangunan, 32(1): 163-174.